Yesterday, Tammy Tolleson Knee (the new director of the Phyllis J. Washington Center for the Advancement of Positive Education) and I arrived in Kalispell, Montana for a 2+ day retreat with staff from the Nate Chute Foundation (NCF). Their mission: The Nate Chute Foundationsupports, educates and empowers our community to promote mental wellness and reduce suicide. You can learn more about NCF’s fabulous work and staff right here: https://www.natechutefoundation.org/
Our retreat is top secret, but I’ll share it here anyway because I don’t like secrets.
Having grown weary with traditional, pathology-oriented approaches to “suicide prevention” we’re working together to create a new curriculum tentatively titled “Strengths-Based Suicide Education for Concerned Adults.” Our plan is to use this new curriculum to replace all the unhelpful and sometimes traumatizing approaches to suicide prevention.
Yes, we have big goals.
Today we’re breaking away from our retreat for a short presentation/consult with Immanuel Living of Kalispell.
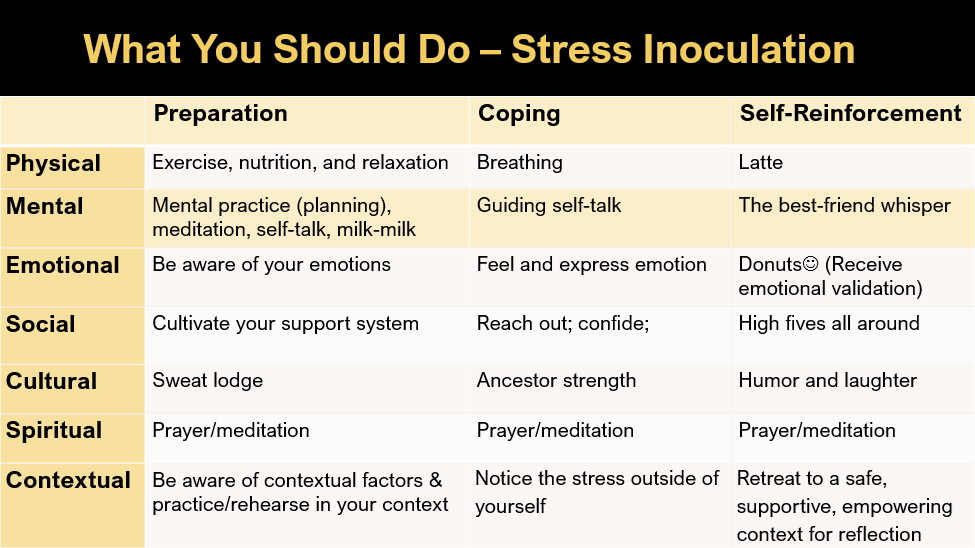
In preparation for this short conversation, I pulled out an old slide about a thing called Stress Inoculation Training (thanks Don Meichenbaum!).
The point of SIT is to prepare for stressors or provocations in life that adversely affect us. For example, let’s say that you find ___________ stressful. (You can put anything in the blank. It could be exercise, talking with your boss, going to church, not going to church, speaking in public meetings, etc.). Then you create your own personalized stress inoculation plan.
Meichenbaum’s therapy approach is designed to prep or inoculate us from our usual and predictable stressors. He described three steps: (1) preparation for provocation, (2) coping with the provocative situation, and (3) reflection and self-reinforcement. Here’s a visual, with our stressors and responses organized into 7 dimensions:
If we all had rational brains and lived in a rational world, SIT would work perfectly for everyone. But like everything, it doesn’t always work. During today’s talk, I’m revealing the secrets of why our best laid plans often fail. Newsflash: it has to do with our quirky brains, which, although amazing, also automatically and regularly take us down into negative thinking rabbit holes.
TBH, IMHO, dipping into a negative thinking rabbit hole every once in a while can be fun, but if your intention was to avoid negative thinking rabbit holes, they’re considerably less fun.
Unfortunately, due to time limits and the need for mystery in marketing, this blog is ending without me sharing the five secrets of why our pesky brains often derail us from our positive intentions. Sorry about that. They’re in the pdf of the ppts linked below, and although you can find them there, it’s much more fun for us to talk about these in person . . . so I hope to see you at a presentation in the future.
Along with Kimberly Parrow, this morning I have the privilege of offering a 3-hour workshop at the 2026 ACA Annual Conference.
As always, this is a challenging topic. But in the spirit of a strengths-based approach, it’s important to remember that by engaging in this learning together, we make ourselves stronger, more capable, and more prepared to help clients and students who are feeling suicidal.
Thanks to ACA for the opportunity, to Kim for the help, and for the attendees for being rockstars who are dedicated to helping individuals who are experiencing immense emotional pain and struggling with suicide. You are amazing.
All too often on this blog I’m writing about what I’m doing and I’m thinking. I suppose that’s just fine, after all, it’s my blog. But, as many people have said before me and better than I can, “Other people matter” and seeing the light (or the divine) in others is among the most meaningful experiences we can have.
One light I’ve been seeing lately is the strengths-based suicide prevention work that the Firekeeper Alliance (a non-profit org) is doing on the Blackfeet Reservation in Northern Montana. In July, they had a “suicide prevention” heavy metal concert called Fire in the Mountains, complete with amazing metal bands and equally amazing panels, discussions, and speakers. If you’re interested in creative approaches to well-being, you really should check them out.
This past Thursday, Charlie Speicher, architect of the Firekeeper Alliance and Director of the Buffalo Hide Academy in Browning, shared one of their Suicide Prevention Month activities. The idea is simple: Feature the beauty and strengths of the reservation and its people. The product: A 12-minute video that focuses on what gives the Blackfeet people hope. The video captures the faces, sentiments, and emotions in response to “What gives you hope?” Here’s the link on Youtube:
All too often, people think and share information about the challenges of reservation life. This video shares hope, beauty, and potential.
With your help, I hope this video travels far and wide. Please share. At the very least, it should get all over Montana media. And, just in case anyone has the right connections, I think it’s a great fit for virtually any national media outlet that wants to shift toward a positive narrative in Indian Country.
Thanks for reading . . . and for seeing the light (and fire) in others.
Why Do We Need a Strengths-Based Approach to Suicide Assessment and Treatment?
Imagine this: You’re living in a world that seems like it would just as soon forget you exist. Maybe your skin color is different than the dominant people who hold power. Maybe you have a disability. Whatever the case, the message you hear from the culture is that you’re not important and not worthy. You feel oppressed, marginalized, unsupported, and as if much of society would just as soon have you become invisible or go away.
In response, you intermittently feel depressed and suicidal. Then, when you enter the office of a health or mental health professional, the professional asks you about depression and suicide. Even if the professional is well-intended, judgment leaks through. If you admit to feeling depressed and having suicidal thoughts, you’ll get a diagnosis that implies you’re to blame for having depressing and suicidal thoughts.
The medical model overfocuses on trying to determine: “Are you suicidal?” The medical model is also based on the assumption that the presence of suicidality indicates there’s something seriously wrong with you. But if we’re working with someone who has been or is currently being marginalized, a rational response from the patient might be:
“As it turns out, I’ve internalized systemic and intergenerational racism, sexism, ableism, and other dehumanizing messages from society. I’ve been devalued for so long and so often that now, I’ve internalized societal messages: I devalue myself and wonder if life is worth living. And now, you’re blaming me with a label that implies I’m the problem!”
No wonder most people who are feeling suicidal don’t bother telling their health professionals.
When I think of this preceding scenario, I want to add profanity into my response, so I can adequately convey that it’s completely unjust to BLAME patients for absorbing repeated negative messages about people who look like or sound like or act like them. WTH else do you think should happen?
This is why we need to integrate strengths-based principles into traditional suicide assessment and prevention models. Of course, we shouldn’t use strengths-based ideas in ways that are toxically positive. We ALWAYS need to start by coming alongside and feeling with our patients and clients. As it turns out, if we do a good job of coming alongside patients/clients who are in emotional pain, natural opportunities for focus on strengths and resources, including cultural, racial, sexual, and other identities that give the person meaning.
I’m reminded of an interview I did with an Alaskan Native person from the Yupik tribe. She talked at length about her depression, about feeling like a zombie, and past and current suicidal thoughts. Eventually, I inquired: “What’s happening when you’re not having thoughts about suicide?” She seemed surprised. Then she said, “I’d be singing or writing poetry.” I instantly had a sense that expressing herself held meaning for her. In particular, her singing Native songs and contemporary pop songs became important in our collaborative efforts to build her a safety plan.
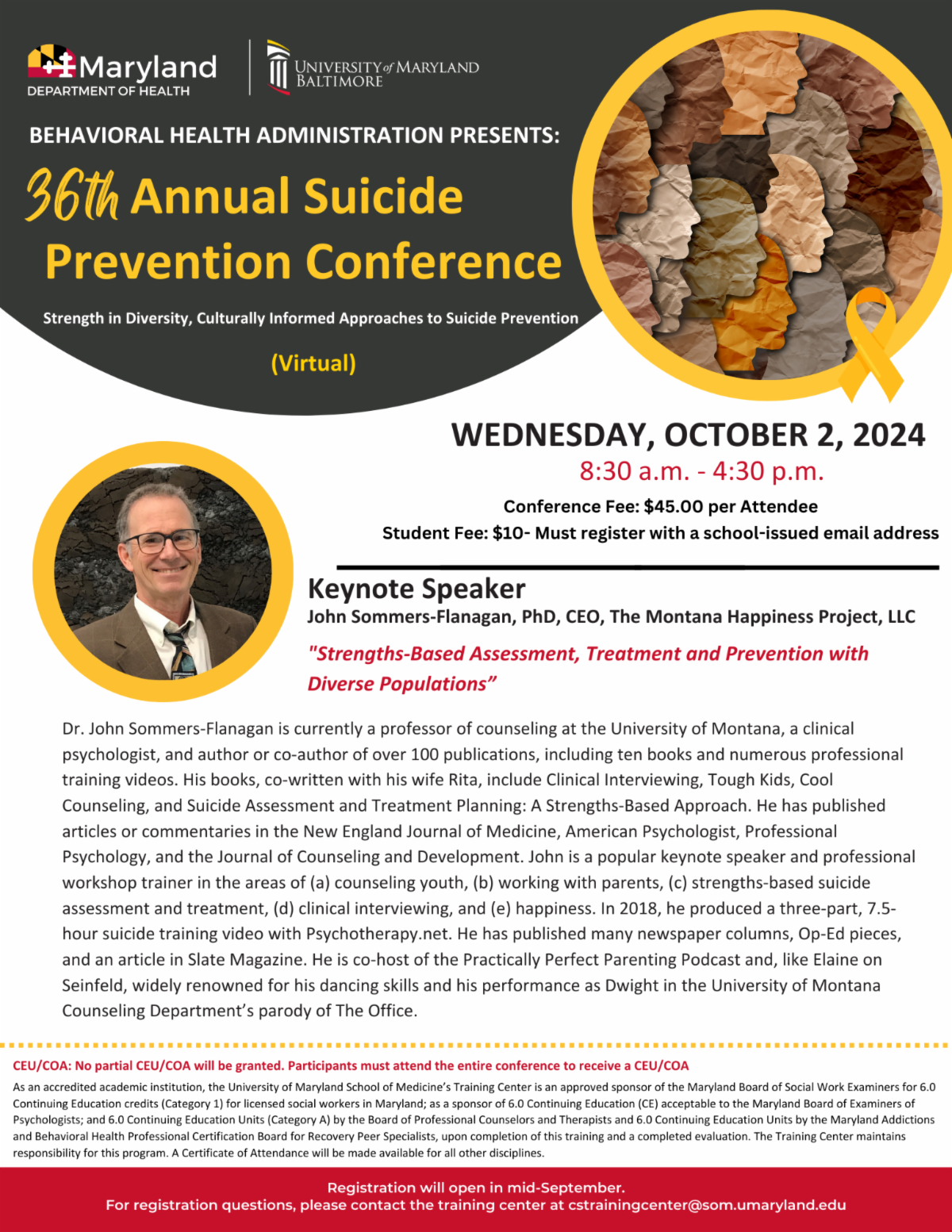
This coming Wednesday morning I have the honor of presenting as the keynote speaker for the Maryland Department of Health 36th Annual Suicide Prevention Conference. During this keynote, I’ll share more ideas about why a strengths-based model is a good fit when working with diverse clients who are experiencing suicidal thoughts and impulses.
With all that said, here’s the title and abstract of my upcoming presentation.
Strengths-Based Assessment, Treatment, and Prevention with Diverse Populations
Traditional suicide assessment tends to be a top-down information-gathering process wherein healthcare or prevention professionals use questionnaires and clinical interviews to determine patient or client suicide risk. This approach may not be the best fit for people from populations with historical trauma, or for people who continue to experience oppression or marginalization. In this presentation, John Sommers-Flanagan will review principles of a strengths-based approach to suicide prevention, assessment, and treatment. He will also discuss how to be more sensitive, empowering, collaborative, and how to leverage cultural strengths when working with people who are potentially suicidal. You will learn at least three practical strengths-based strategies for initiating conversations about suicide, conducting culturally-sensitive assessments, and implementing suicide interventions—that you can immediately use in your prevention work.
When I wrote this, I was listening to Dr. Jennifer Crumlish, a consultant for the CAMS-Care program. Dr. Crumlish provided a fantastic overview of the challenges associated with suicide prevention and interventions, along with introductory information pertaining to implementing the CAMS model. For more on CAMS-Care, see this link: https://cams-care.com/
Earlier in the day, Leah Finch—one of our excellent doc students in counseling—and I, did our presentation. Our participants were awesome. A bit later, I got to be on an “expert panel” along with several very cool people, facilitated by Dr. Jen Preble. We fielded an array of interesting questions from the audience. Very fun.
For those of you interested, here are the ppts Leah and I developed, here they are:
Yesterday I had a chance to do a 3-hour online workshop with a very cool group of about 22 smart, skilled, and dedicated professionals. They engaged with the content and consequently, we had some great discussions. One of the discussions has kept percolating for me today. The topic: How do we handle situations where clients are clearly suicidal, but are reluctant or unwilling to develop and agree to a collaborative safety plan.
We talked about how, often, the knee-jerk impulse is to pursue hospitalization. While that’s a viable and reasonable option, the problem is that hospitalization and discharge is a notable risk factor for death by suicide. The other problem is that it’s pretty much impossible for us to know if the client’s resistance to a safety plan indicates increased risk, or just resistance to what s/he/they view as a coercive mandate.
There’s no perfect clinician response to this dilemma. Hospitalization helps some clients, and causes demoralization and regression in others. Not hospitalizing can feel too risky for practitioners.
We talked about a few guidelines in dealing with this conundrum. They include: (a) consulting with colleagues, (b) reflecting on the client’s engagement in other aspects of treatment (increased engagement in treatment is a protective factor), (c) evaluating client intent and client impulsivity, and (d) documenting your decision-making process (including citations indicating that psychiatric hospitalization may not be the best alternative). But again, there’s no perfect guideline.
When discussing Kate’s situation and other scenarios that involve outpatient work with highly suicidal clients, the following question usually comes up, “What if your judgment is wrong and she either makes a suicide attempt, or she kills herself before your next session?” This is a great question and gets to the core of practitioner anxiety.
The answer is that, yes, she could kill herself, and if she does, I’ll feel terrible about my clinical judgment. Also, I might get sued. And, if I’m inclined toward suicidal thoughts myself, Kate killing herself might precipitate a suicidal crisis in me. Sometimes suicide tragedies happen, and sometimes we will feel like the tragedy was our fault and that we should have or could have prevented it. That said, most suicides are more or less unpredictable. Even if you think you’re correct in categorizing someone as high or low risk, chances are you’ll be wrong; many high-risk clients don’t die by suicide and some low-risk clients do (see Sommers-Flanagan, 2021, for a personal essay on coping with the death of a client to suicide; https://www.psychotherapynetworker.org/magazine/article/2565/the-myth-of-infallibility).
More depressing is the reality that hospitalization – the main therapeutic option we turn to when clients are highly suicidal – isn’t very effective at treating suicidality and preventing suicide (Large & Kapur, 2018). Hospitalization sometimes causes clients to regress and destabilize, and suicide risk is often higher after hospitalization (Kessler et al., 2020). Because hospitalization isn’t a good fit for many clients who are suicidal and because we can’t predict suicide very well anyway, some cutting edge suicide researchers recommend intensive safety planning as a viable (and often preferred) alternative to hospitalization. In the case of Kate, as long as she’s willing to collaborate, and I’m able to contact her husband, and we can construct a plan that provides safety, then I’m on solid professional ground (or at least as solid as professional ground gets when working with highly suicidal clients).
Kessler, R. C., Bossarte, R. M., Luedtke, A., Zaslavsky, A. M., & Zubizarreta, J. R. (2020). Suicide prediction models: A critical review of recent research with recommendations for the way forward. Molecular Psychiatry, 25(1), 168-179. doi:http://dx.doi.org/10.1038/s41380-019-0531-0
Large, M. M., & Kapur, N. (2018). Psychiatric hospitalisation and the risk of suicide. The British Journal of Psychiatry, 212(5), 269-273.
The idea that healthcare professionals must take an authoritarian role when evaluating and treating suicidal clients has proven problematic (Konrad & Jobes, 2011). Authoritarian clinicians can activate oppositional or resistant behaviors (Miller & Rollnick, 2013). If you try arguing clients out of suicidal thoughts and impulses, they may shut down and become less open.
For decades, no-suicide contracts were a standard practice for suicide prevention and intervention (Drye et al., 1973). These contracts consisted of signed statements such as: “I promise not to commit suicide between my medical appointments.” In a fascinating turn of events, during the 1990s, no-suicide contracts came under fire as (a) coercive and (b) as focusing more on practitioner liability than client well-being (Edwards & Sachmann, 2010; Rudd et al., 2006). Suicide experts no longer advocate using no-suicide contracts.
Instead, collaborative approaches to working with suicidal clients are strongly recommended. One such approach is the collaborative assessment and management of suicide (CAMS; Jobes, 2016). CAMS emphasizes suicide assessment and intervention as a humane encounter honoring clients as experts regarding their suicidal thoughts, feelings, and situation. Jobes and colleagues (2007) wrote:
CAMS emphasizes an intentional move away from the directive “counselor as expert” approach that can lead to adversarial power struggles about hospitalization and the routine and unfortunate use of coercive “safety contracts.” (p. 285)
In the piece I review some information and make one point that I’d like to share more broadly. Below are several opening paragraphs from the Op-Ed piece.
*Beginning of Excerpt*
Beyond Suicide Prevention: The Montana Happiness Challenge
John Sommers-Flanagan, Ph.D.
All September, organizations and individuals celebrated suicide prevention month, sharing information about suicide and promoting strategies for preventing suicide deaths. Although the information was life-affirming, underneath the messaging lies an unpleasant truth: Broadly speaking, suicide prevention has been failing for over two decades.
In August, the Centers for Disease Control (CDC) released provisional United States suicide data for 2022. The news was bad. An estimated 49,449 Americans died by suicide in 2022—the highest number ever recorded in U.S. history.
The bad news goes far beyond last year. Suicide rates have risen every year for over 20 years, with only two puzzling exceptions. In 2020 and 2021—during the onset of COVID-19, lockdowns, and other national stressors—suicide rates declined; they declined despite the fact that by every other measure Americans were suffering from unprecedented stress, depression, anxiety, and suicidal thinking. Suicide researchers have long noted this odd pattern: higher stress, depression, anxiety, and suicidal thinking do not inevitably translate to more suicides.
If all this seems confusing—20 years of vigorous suicide prevention, and suicide rates steadily rise, while during 2 years of intensive COVID-related individual and public distress, suicide rates go down—it’s only because it is.
In his book, Rethinking suicide, Craig Bryan, a renowned suicide researcher, called suicide “a wicked problem,” noting, “Wicked problems cannot be definitively solved or completely eliminated . . .” In fact, as Bryan and others have described, efforts to eliminate wicked problems sometimes make them worse. The preceding facts don’t indicate suicide prevention doesn’t work . . . and they don’t mean COVID pandemics solve the suicide problem. What they do mean—at minimum—is that suicide prevention doesn’t work for everyone, and we need to collectively think differently about this wicked problem.
Suicide prevention ideology over-focuses on eliminating “bad” or negative thinking and behavior. This conceptualization is contrary to science and common sense. The science says that telling people to stop engaging in unhealthy behaviors usually doesn’t work. When people are judged and told they should change, they often become defensive and more resistant to change. This is human nature.
All this brings me to share one strategy for moving beyond traditional suicide prevention. We should put more energy into growing and nurturing positive and meaningful thoughts and behaviors. People are more likely to change if they’re accepted for who they are, and then invited to try something interesting.
*End of Excerpt*
If you read the preceding and have a reaction, I’d love to hear your thoughts on how, with increasing suicide prevention focus, the suicide deaths keep increasing, and why, during the two worst years of COVID, suicide deaths decreased. Feel free to post on this blog or pop me an email.
This week, for the Montana Happiness Challenge, we’re focusing on adopting a mindset where we look for joy or for what inspires us. Last week I did a day-long training on Suicide Assessment and Treatment with professionals in Canada. At the end of the day, I was inspired that they took a full-day to learn about something so hard and challenging. Similarly, if you got through this whole blog because of your interest in making the world a better place, you inspire me.
If you want to keep up with the Montana Happiness Challenge, here are some clickable options:
While engaged in a little late-night Twitter scrolling, I came across a fascinating post and thread questioning the utility of suicide screening for low risk populations (e.g., schools). Having been mildly opposed (along with the UK and Canada), to general population suicide screenings, I felt validated, especially upon discovering that Craig Bryan was author of the Twitter thread. Dr. Bryan is one of the best and most authoritative resources on suicide in the world. As of two nights ago, I was only familiar with his professional book with David Rudd (Brief cognitive-behavior therapy for suicide prevention) and his excellent work with military veterans, suicide, and lethal means management. I also knew he had recently published a new book titled, “Rethinking Suicide.”
Then, today, I checked out Rethinking Suicide online. I was gob smacked. It’s fantastic.
This post is mostly to pitch Craig Bryan’s book.
Among other gems, Dr. Bryan frames suicide prevention as a “wicked problem” and tells us about the origin of the term, wicked problem. What’s not to love about that.
Here’s a quote from his introduction: “Consistent with the perspective of suicide as a wicked problem, I will argue in this book that we need to replace our solution-based approach to suicide prevention with a process-based approach focused on creating and building lives worth living” (p. 7). Wow. That’s like music to my ears.
Dr. Bryan also weaves in “confirmation bias” (more music) as part of his critique of using so-called “mental illness” as an explanatory mechanism in suicide (I know if you know me and this blog, you know I don’t even use the term mental illness unless I’m explaining why I don’t use the term mental illness, and so I’m destined to love Dr. Bryan’s deconstruction of that concept).
Anyway, you can find Rethinking Suicide through your favorite online bookseller. I recommend it highly. I’ve ordered my copy. It’s about time we all started rethinking suicide.
After facing an overwhelming number of choices on Black Friday and Cyber Monday, now we’re faced with another litany of excellent choices for Giving Tuesday. There are so many wonderful charities to support. You can’t go wrong with supporting food banks, shelters, and other organizations that push back against poverty. You also can’t go wrong supporting children, minorities, education, and the environment . . . these are all huge needs.
Along with the preceding charity types, this year Rita and I are wholeheartedly supporting college student mental health. We’ve seen the struggles firsthand and we believe college students can benefit from greater access to mental health services. Specifically, we’re supporting a University of Montana Foundation project called “The University of Montana Mental Health and Happiness Fund.” We see the University of Montana Mental Health and Happiness Fund as a win-win-win. Here’s why.
The first win is that the funds will go to provide more hours of mental health counseling for college students. Unfortunately, more than ever before, college students are stressed and experiencing mental health struggles. These struggles can include suicidal thoughts and behaviors. As far as age groups vulnerable to death by suicide, the college student age group is among the highest (along with older males). Supporting college student mental health can literally save lives and help college students graduate and become significant contributors to their communities. Currently, Counseling Services at the University of Montana needs more counselors to meet increased needs.
The second win is about “workforce development.” In Montana, and around the nation, we need a continuous flow of competent and capable mental health professionals. That’s why the first priority of the University of Montana Mental Health and Happiness Fund is to support a ½ time Counseling Intern for UM’s Counseling Services department. Funding an intern means that the intern gains valuable experience and supervision and can then go out and contribute to mental health in the community. If we receive more funds than expected, we will either fund a second ½ time counseling intern or we will fund happiness promotion projects at UM and within the Western Montana area.
The third win is basic economics. College students contribute to local economies. When they graduate, college students also create capital. College students become entrepreneurs, scientists, grant writers, community leaders, parents, and grandparents. In all these roles, college graduates will do better and be better if they have better mental health.
Our 2021 fundraising goal is $45,000. We’ve already raised over $22,000. Please help us reach our goal so we can contribute to positive mental health and happiness at the University of Montana.
If you’re interested in joining Rita and me in supporting the University of Montana Mental Health and Happiness fund here are the instructions.
Good morning! The 2021 MHA Suicide Summit has started (see below) and I’ll be up in less than an hour.
Sometimes I think the hardest part about doing workshops is writing the workshop blurb. My problem-and maybe it’s just my problem—is that the process of writing workshop blurbs nearly always impairs my judgment. I start out writing like a sensible and rational person, but eventually I decompensate into displaying delusions of grandeur. For the Mental Health Academy Suicide Summit, I completely lost touch with reality and claimed that I would,
Describe strengths-based principles for suicide assessment and treatment
Be able to implement three strengths-based assessment tools (and recognize the limits of risk and protective factor assessment)
Identify suicide drivers (and goals) linked to seven common life dimensions
Describe at least one wellness and mood management positive psychology strategy for patients and practitioners.
Of course, all of this is great, but, here’s the catch. I’m only presenting for 45 minutes!
If anyone out there can help me become more realistic, I would appreciate the input.
In the meantime, here are the ppts for the presentation today.