
All too early tomorrow morning I’ll be doing a couple presentations for medical staff at the Community Medical Center in Missoula. Despite the early hour, I look forward to some interesting and useful conversations with the staff. This link is to a very long ppt slide deck. It’s long because the two groups with which I will work are small, and so I will do portions of the slides depending on what the groups would like to cover. Here’s a pdf of the ppts!
All posts by johnsommersflanagan
More Thoughts on Suicide Prediction and Suicide Screening (from Craig Bryan, Ph.D.)
Hi All,
Below, I’ve a pasted LinkedIn post from Dr. Craig Bryan, author of “Rethinking Suicide” and a leading suicide researcher. At the bottom of his comments there’s a link to the article of which he speaks.
Enjoy!
*****************
From Craig Bryan, LinkedIn – 6/29/2026
We keep trying to predict who will attempt suicide. A 15-year study suggests we’re asking the wrong question.
Researchers followed 2,060 Brazilian children from age 10 into their mid-twenties—one of the longest prospective suicide studies ever conducted outside a high-income country. They measured genetics, perinatal history, family psychiatric illness, childhood adversity, cognition, and clinical symptoms, then tested all of it together against who later attempted suicide.
The result: even with multiple domains of risk factors combined, prediction accuracy stayed modest (AUC 0.665), barely above the ceiling seen across 50 years of suicide research. More sophisticated machine learning models didn’t do any better than simple logistic regression.
Three factors stood out as consistent, actionable, and population-relevant: childhood threat exposure (especially bullying), caregiver history of suicide attempts, and childhood externalizing disorders. Bullying alone accounted for the largest share of preventable risk in the entire study.
The authors’ conclusion is blunt: distal childhood risk factors will likely never predict individual suicide attempts with precision, because suicide is driven by acute, fast-moving processes that a baseline assessment can’t capture. Trying to screen our way to safety has a ceiling. We hit it decades ago.
The better investment may not be sharper prediction. It may be quieter, structural prevention like anti-bullying programs, supporting parents with histories of suicidal behavior, and early identification of behavioral disorders, the kind of intervention that helps a population, whether or not we ever know which child needed it most.
**************************
Here’s the article link: https://lnkd.in/eRWtBiXK
I’m excited about Dr. Bryan’s post not because of the difficulties with prediction (which we’ve long know), but because of the idea of moving upstream toward structural prevention. I also feel this fits really well with what we’re trying to do with CAPE.
Obviously, I love this quotation: “Trying to screen our way to safety has a ceiling. We hit it decades ago.”
Have a great evening!
JSF
How to Grow Wellbeing in Teachers and Schools
I’m at the Office of Public Instruction Summer Institute in Bozeman today (and tomorrow), along with the Pirate and the Pusher. The Summer Institute is an annual four days of training for Montana educators.
Shortly after arriving, two women sitting at a table stared at me, looked away, and then stopped me as I walked by, saying, with enthusiasm, “We just took your class!”
They were, of course, referring to our Happiness for Educators course. Although completely online, I’m presenting in many of the videos, sometimes in my pajamas. We were all excited to meet in person.
They also got to meet Dylan Wright (who plays the role of a pirate in our Happiness for Educators course). I mean, how can you have a Happiness for Educators course without a pirate? They also met Tammy Tolleson Knee, the new and fabulous director of the Phyllis J. Washington Center for the Advancement of Positive Education at the University of Montana and high leverage “Pusher” of all things positive.
Tomorrow will be even more excitement. I have the honor of delivering the morning keynote. I’ll be opening with a make-believe scenario, with me as a candidate for governor. I’ve done this a few times previously during presentations for educators. It’s a method I use for emphasizing the central and foundational role that educators and education play in society.
My platform as a candidate for governor of Montana is education . . . education . . . and education . . . because. . .
The road to a good economy goes through education.
The road to a healthy enviroment goes through education.
The road to a civil society goes through education.
The road to excellence in health care goes through education.
The road to justice goes through education.
I could go on, but I think you get the point. As John Adams, founding father and our 2nd president once said (I’m paraphrasing), “It’s impossible to spend too much money on public education.”
And so, yes, there will be more excitement tomorrow because it doesn’t get much better than spending a day with 400 Montana educators who are dedicated to helping young people become educated citizens.
I’m posting ppts of my two presentations (keynote and workshop) below.
Who is Dr. Sonja Lyubomirsky?
From Wikipedia: Sonja Lyubomirsky is a Russian-born American professor in the Department of Psychology at the University of California, Riverside and author of The How of Happiness: A Scientific Approach to Getting the Life You Want.
And there’s so much more.
Not long ago, Tammy Tolleson Knee, the new Director of the Phyllis J. Washington Center for the Advancement of Positive Education, asked me if I thought she should attend the Western Positive Psychology Conference at Claremont Graduate University. I saw that Sonja Lyubomirsky was the featured keynote speaker and immediately said “Hell, Yes!” [I didn’t really swear at the time, but it sounded cooler for this blog post].
I also looked at my calendar and was bummed that I couldn’t attend. But then I said to Tammy that we should reach out to Dr. Sonja for a possible short meet-up at the conference.
So I did.
She responded within hours.
At the conference, Tammy got to meet her and talk–despite the fact that Dr. Sonja also was busily signing her new book for the masses. How cool!
And then, Tammy shared the following email with our whole CAPE staff upon her return.
Happy Friday, ,
In honor of my Sonja Lyubomirsky buzz, I thought I’d share some fun tidbits and resources from the WPPA conference!
- Her last name is pronounced Lou – Boe – Mere – Ski
- Here is a recent chapter she co-authored in the Handbook of Social Psychology(6th ed.) titled “Well-being” (though she prefers the term “happiness”). It’s long but comprehensive.
- Here is a 5-minute Ted Talk teaser on her new book.
- Fun fact: She has been cited in academic publications more than 90,000 times.
- She said the Big 3 PPIs are Gratitude, Kindness, and Social Interventions (or Acting Extraverted).
- Among the many fascinating findings she shared was a study from Brain, Behavior, and Immunity suggesting that intentionally engaging in more extroverted behavior can improve patterns of gene expression.
- She joked that part of her wishes they had never introduced the happiness pie. More on that later.
- Her final advice: Share deeply, listen and be curious.
- My overall takeaway: There is no end to what we can learn in positive psychology, and CAPE is very much on the right track.
In conclusion: Who is Dr. Sonja Lyubomirsky? She’s a bad-ass academic researcher who’s also incredibly personable and who, in her spare time, writes books designed to help people live better lives. You can learn more about her here: https://sonjalyubomirsky.com/
The 4th Edition of Counseling and Psychotherapy Theories in Context and Practice is Now Available
Rita and I got our copies in the mail two days ago. Thanks to Bryan Cochran, the book is better than ever, and the cover is more beautiful than ever. Bryan asked Brian Christianson, a local photographer in Missoula, Montana permission to use one of his photos and, wow, it looks great.
The feeling of opening a box, getting out a book, and holding it in my hands never gets old. And, when the book has your name on it, the feelings are magnificent.
I feel like Steve Martin in the old classic film, The Jerk, when he gets a new phone book and finds his name in it.
Our books are for students in the mental health professions and mental health professionals, so they will never be bestsellers. Nevertheless, we get some sweet, meaningful, and validating feedback—which I treasure. Here’s the latest, forwarded to me by a former doctoral student at the University of Montana who is now a professor and who is already using our book (which is very kind and affirming). One of her students wrote,
“. . .let them know their text is easy to digest and has this magical ability to pull the reader in. There are moments in the first chapter where I felt like I was part of the authors’ lived experience. That feeling makes it easy to read and learn! I have enjoyed the text so far.”
Hopefully the magic will continue beyond the first chapter.
I’ll try to be more consistent in posting a few excerpts from the book on this blog. . .despite the fact that I’m not all that great at consistency! If you’re interested, you can find the text online.
Have a great weekend.
John SF
The Future of Mental Health Awareness (Month)

I wrote my reflections on mental health awareness and prevention as an Op-Ed piece and pasted it below.
The Future of Mental Health Awareness
As we exit Mental Health Awareness Month version 2026, I’m already anticipating May 2027. It’s time to rethink, rebrand, and reboot mental health awareness and prevention.
Think about it. Can you name a single mental disorder that, in your lifetime, has decreased in significance?
Depression? Anxiety? ADHD? Bipolar? As a mental health professional for the past 45 years, I’ve watched mental disorders in America stubbornly increase, despite more national, state, and local mental health awareness and prevention programs than ever before.
Mental health awareness and prevention are failing for multiple reasons, none of which are the fault of all the compassionate, hard-working, and well-intended people involved with mental health prevention. More likely, our collective failure begins with confusion over how to define mental health. Most Americans use “mental health” to describe mental health problems, mental disorders, or mental illness. Mental health is supposed to be positive and include joy, happiness, meaning, and mutually supportive relationships.
Instead, even the term “mental health prevention” is awkwardly phrased. Wait. Does mental health prevention mean we’re preventing mental health? Ironically, that might be exactly what we’re doing.
Without a positive vision of mental health, we’re left trying to manage, eliminate, or run from negative symptoms. Mental health should be something positive to strive toward. How about we start with the World Health Organization’s (WHO) definition of mental health? “A state of mental well-being that enables people to cope with the stresses of life, realize their abilities, learn and work well, and contribute to their community.”
Pretend for a moment that you’re a young person. You have two options. You can enroll in a program designed to reduce your anxiety and depression. Or you can enroll in a program designed to help you strive toward happiness, meaning, and realizing your abilities. Of course, this is a false dichotomy, but which direction do you find more hopeful and inspiring?
We also need to stop using unidimensional slogans to bludgeon community mental health from bad to better. Mental health awareness is a great example. Too much awareness of negative symptoms is not a good thing. More on this soon.
Research indicates that school-based mental health programs can adversely affect students. Providing prevention programming that simultaneously helps all students is a worthy, but unrealistic goal. Because preference is a powerful determinant of effective therapy, students might be better served by choosing from a menu of indirect mental health education activities.
Contemporary prevention programs also ignore several basic psychological principles.
When young people begin learning about mental disorders, a natural and powerful process begins. First, they learn about psychiatric symptoms. Then, they’re told these symptoms represent mental illnesses. Inevitably, they see these symptoms in themselves (or their friends) and begin self-diagnosing. Sometimes, the labels help explain their experiences and youth experience temporary relief. Who’s not reassured to learn that social anxiety is a thing? But, when the label gets too closely linked to identity, diagnosis becomes self-limiting. Students think: “I can’t pay attention because I have ADHD” or “My anxiety stops me from having fun and being around people.” And, because labels are sticky, it becomes difficult for young people (and adults) to shake the label and pursue their potential.
As you read these words, thousands of American youth are learning about their so-called mental disorders in at least two ways: on social media (via Tik-Tok, in particular) and through school-based mental health literacy/awareness workshops. More awareness and more information can make mental health worse—especially if the information is inaccurate or not applied with sensitivity and nuance.
Another psychological principle operates to sustain and deepen negative labeling. Like everyone, young people are inclined toward “confirmation bias.” They easily find evidence for their pre-existing beliefs while discarding evidence inconsistent with their pre-existing beliefs. If I believe I have anxiety and my anxiety limits my ability to participate in social activities, I will become skilled at noticing when my anxiety is adversely affecting me, while dismissing evidence that I’m strong and resilient enough to socialize with my peers.
What we pay attention to grows. Although my teenage clients would respond to this statement with “duh,” prevention programs ignore this concept by paying far too much attention to what’s wrong. We will not shrink problems by paying more attention to them. This is fundamental brain science. The more we focus on and talk about our problems, the better we become at focusing on and talking about our problems. The famous neuroscientist Donald Hebb put it this way: “Neurons that fire together, wire together.” The more we think about our problems, the more we’re teaching our brain to think about our problems. Soon, it becomes automatic, and you’ll be thinking about your problems all day long.
For 2027, let’s reboot mental health. Let’s redefine mental health as a positive emotional, psychological, and relational state. Then, let’s help young (and older) people develop strengths, skills, empathic relationships, positive experiences, and resources to successfully pursue positive mental health.
Together, we can turn Mental Health Awareness Month into a collective experience of joy and wellbeing for everyone.
********************************************
John Sommers-Flanagan, Ph.D. is a clinical psychologist and founding director of the Phyllis J. Washington Center for the Advancement of Positive Education at the University of Montana. He is coauthor of 10 books and many professional articles. The opinion expressed here is solely that of John Sommers-Flanagan and does not represent his current or former employers. You can email your thoughts to: john.sf@mso.umt.edu. For more information, go to https://johnsommersflanagan.com/ or https://www.umt.edu/education/cape
Mental Health Awareness, Happiness for Educators, a Free “Good Day for Educators” in Missoula, and More
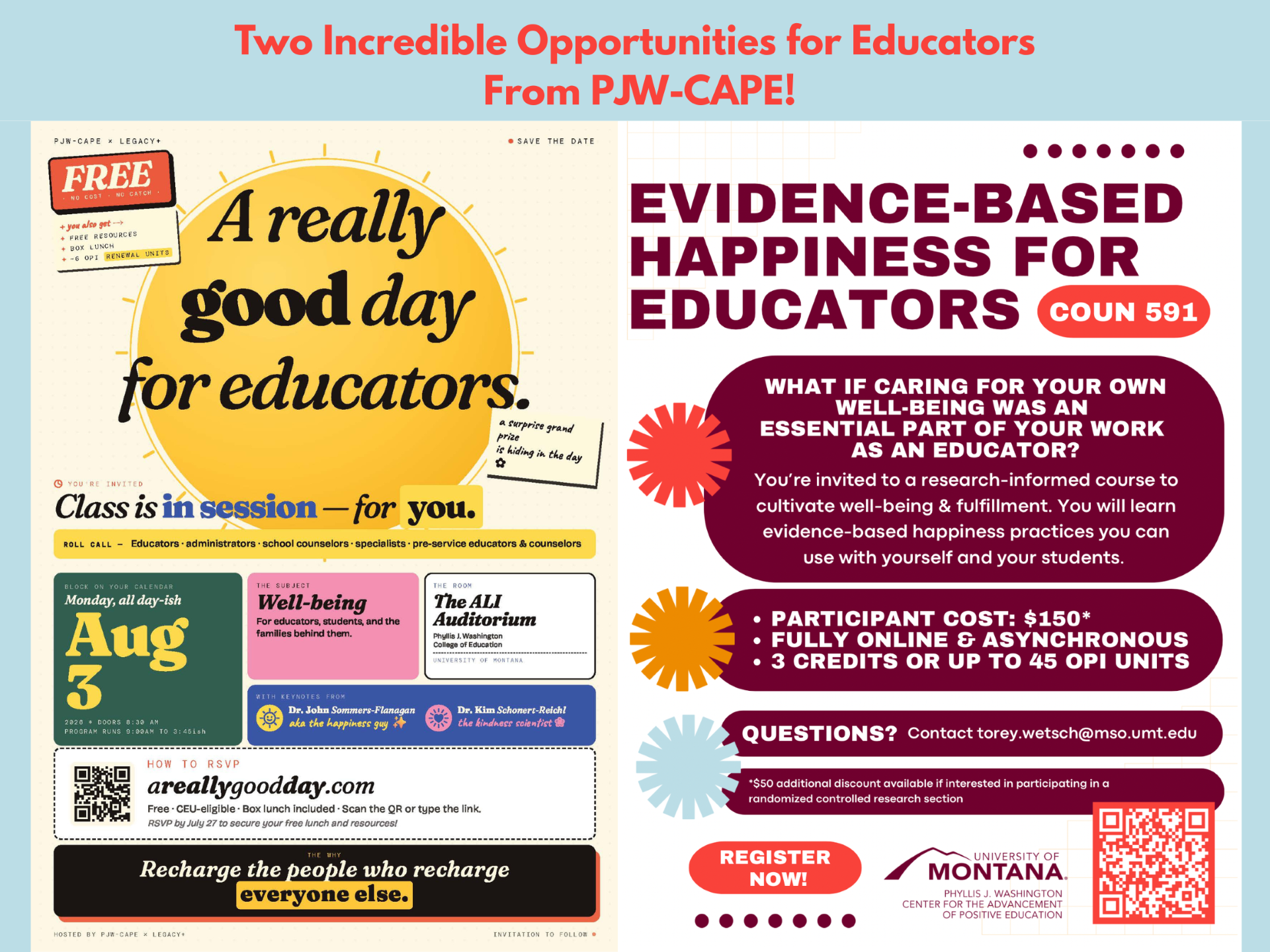
At the Phyllis J. Washington Center for the Advancement of Positive Education at the University of Montana we have two big and exciting activities happening this summer.
The first one is called “A Really Good Day for Educators.” We’re offering this FREE, live and in-person day of training for educators on August 3 in Missoula in collaboration with a fabulous organization called Legacy+. Legacy+ is a Toronto-based organization that helps bring purpose to life. They’re also fun and amazing collaborative partners. As one example, they immediately claimed the site https://areallygoodday.com/ for our event landing page. Go there now (if you’re interested). You can learn more about Legacy+ here: https://legacyplus.org/about-us/
The second activity is our usual Evidence-Based Happiness for Educators course. We still have openings and the price is an absolute bargain for 3 UM grad credits or 45 OPI license renewal units.
Last thing. I wrote an Op-Ed piece on Mental Health Awareness Month and sent it to the New York Times. I do that sort of thing once in a while when I want to have sort of a lonely-rejection experience. However, the NYT may be ignoring me, but I’m not ignoring myself, because, I have now submitted the Op-Ed to @johnsommersflanagan.com. . .and the johnsommersflanagan website monitor is much kinder and has let me put a link to a pdf of the lightly edited Op-Ed piece here!
This Op-Ed is a little edgy, so please share your thoughts if you like.
Thanks and happy weekend.
John
The Secret Retreat

Yesterday, Tammy Tolleson Knee (the new director of the Phyllis J. Washington Center for the Advancement of Positive Education) and I arrived in Kalispell, Montana for a 2+ day retreat with staff from the Nate Chute Foundation (NCF). Their mission: The Nate Chute Foundation supports, educates and empowers our community to promote mental wellness and reduce suicide. You can learn more about NCF’s fabulous work and staff right here: https://www.natechutefoundation.org/
Our retreat is top secret, but I’ll share it here anyway because I don’t like secrets.
Having grown weary with traditional, pathology-oriented approaches to “suicide prevention” we’re working together to create a new curriculum tentatively titled “Strengths-Based Suicide Education for Concerned Adults.” Our plan is to use this new curriculum to replace all the unhelpful and sometimes traumatizing approaches to suicide prevention.
Yes, we have big goals.
Today we’re breaking away from our retreat for a short presentation/consult with Immanuel Living of Kalispell.
In preparation for this short conversation, I pulled out an old slide about a thing called Stress Inoculation Training (thanks Don Meichenbaum!).
The point of SIT is to prepare for stressors or provocations in life that adversely affect us. For example, let’s say that you find ___________ stressful. (You can put anything in the blank. It could be exercise, talking with your boss, going to church, not going to church, speaking in public meetings, etc.). Then you create your own personalized stress inoculation plan.
Meichenbaum’s therapy approach is designed to prep or inoculate us from our usual and predictable stressors. He described three steps: (1) preparation for provocation, (2) coping with the provocative situation, and (3) reflection and self-reinforcement. Here’s a visual, with our stressors and responses organized into 7 dimensions:
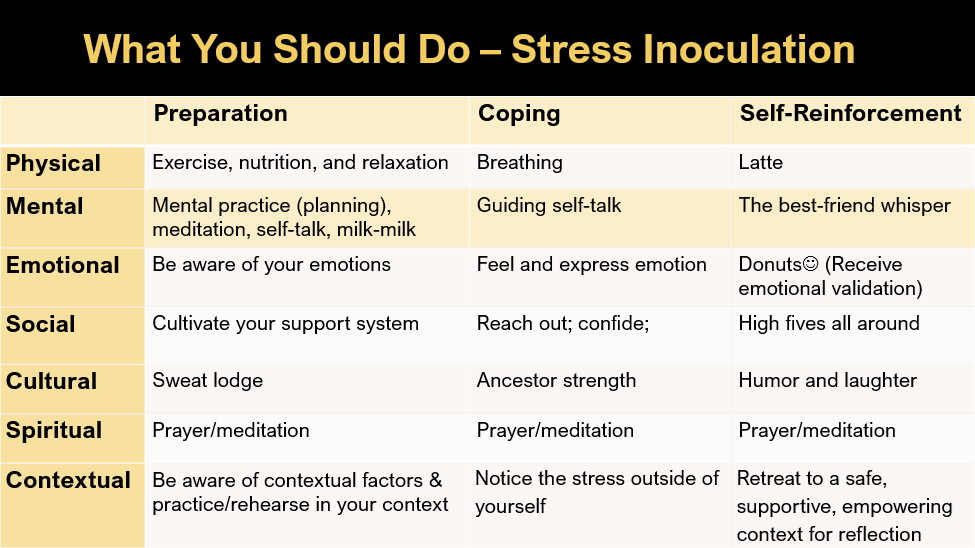
If we all had rational brains and lived in a rational world, SIT would work perfectly for everyone. But like everything, it doesn’t always work. During today’s talk, I’m revealing the secrets of why our best laid plans often fail. Newsflash: it has to do with our quirky brains, which, although amazing, also automatically and regularly take us down into negative thinking rabbit holes.
TBH, IMHO, dipping into a negative thinking rabbit hole every once in a while can be fun, but if your intention was to avoid negative thinking rabbit holes, they’re considerably less fun.
Unfortunately, due to time limits and the need for mystery in marketing, this blog is ending without me sharing the five secrets of why our pesky brains often derail us from our positive intentions. Sorry about that. They’re in the pdf of the ppts linked below, and although you can find them there, it’s much more fun for us to talk about these in person . . . so I hope to see you at a presentation in the future.
Who Is Seth Bodnar?
The following content was published as an Op-Ed piece. I’ve added it here because of access issues. This is a general reflection on Seth Bodnar. Later, I’ll respond to specific questions that have been raised about him. Thanks for reading.
*******************************
In the jungle of social media, I’ve seen many opinions about Seth Bodnar, an independent candidate for U.S. Senate. Because these opinions are often from people who barely know Seth, they’re naturally speculative. In contrast, I’m offering my own admittedly biased perspective. I’ve known, worked with, and been related to Seth for over 22 years.
People have asked, “Why is Seth Bodnar running for the U.S. Senate?” Seth is running for the same reasons he went to West Point, graduated #1 in his class, served in Iraq, and was awarded the Bronze Star and Meritorious Service Medal. The answer: Duty and service.
Seth is guided by an unwavering commitment to service and duty. Unlike some high-ranking military people featured repeatedly in the media, Seth is anti-swagger. He won’t brag about having an Army Ranger Tab, Special Operations Diver Badge, Parachutist Badge, Air Assault Badge, a low golf score, or having been president of Montana’s flagship university. He’ll just get to work so he can be of service.
True, Seth can be boring! If you’re with him in a locker room and hoping for spicy conversations about women or demeaning gossip, you’ll be disappointed. Seth’s idea of locker room talk involves talking over parenting books he’s read, cool research that UM faculty are doing, or macro- and microeconomic concepts (he has two master’s degrees from Oxford University, one in Economic and Social History).
Conversations with Seth usually turn toward how he can become a better father, better leader, better husband, and better person. His self-improvement goals reflect his genuine desire to help other people become the best versions of themselves. He wants a safer, healthier, and economically prosperous Montana for all Montanans, including Indigenous people, farmers, ranchers, veterans, university professors, and everyone else.
You might wonder how I know these things about Seth Bodnar and why I believe in him as a potential United States Senator?
Seth married my stepdaughter, Dr. Chelsea Bodnar. Chelsea is a force in her own right; a Rhodes Scholar, a Harvard-trained pediatrician, and usually one of the smartest people in the room. I could go on about Chelsea’s accomplishments, but this is about Seth and whether he’s U.S. Senate material. Just for the record: Seth chose to marry an equal.
Seth left the military to work at General Electric and have more time with his family. While at GE, Seth often talked about employment that offered him greater meaning and better opportunities to be a positive influence on American youth. So, when the UM presidency became available, I texted him the same day, encouraging him to apply. He said he didn’t think he was qualified. I told him he should apply and let the hiring committee decide. . .and they did.
Seth was my boss at UM for 8 years. I watched as critiques rolled in before he stepped on campus. Morale was low. Enrollment had collapsed. COVID hit. Seth stayed steady. Morale and enrollment improved. He earned our respect, even though university faculty are notoriously cantankerous and critical.
One of Seth’s central values is captured by his UM motto, “Inclusive prosperity.” Let that sink in. For Seth, it means creating meaningful educational and vocational opportunities for everyone, so everyone has a chance for success, and everyone can contribute to the greater state, national and global good.
Seth has a moral compass. I’ve watched him follow that compass for 22 years. His true north is duty and service. He has not and will not favor the elite, engage in degrading locker room talk, or dehumanize other human beings. Period. Seth Bodnar will show up every day ready to work for a more educated, equitable, compassionate, free, and civil society.
********************************************
John Sommers-Flanagan obtained his Ph.D. in psychology from the University of Montana in 1986. He is a former professor in the department of counseling and coauthor of 10 books. The opinion expressed here is solely that of John Sommers-Flanagan and does not represent his current or former employers.
Strengths-Based Suicide for Maryland
Good Morning. In a few minutes I’ll be online with the great people of Maryland. Here’s the ppt for the presentation.
