
All too early tomorrow morning I’ll be doing a couple presentations for medical staff at the Community Medical Center in Missoula. Despite the early hour, I look forward to some interesting and useful conversations with the staff. This link is to a very long ppt slide deck. It’s long because the two groups with which I will work are small, and so I will do portions of the slides depending on what the groups would like to cover. Here’s a pdf of the ppts!
Category Archives: Suicide Assessment and Intervention
More Thoughts on Suicide Prediction and Suicide Screening (from Craig Bryan, Ph.D.)
Hi All,
Below, I’ve a pasted LinkedIn post from Dr. Craig Bryan, author of “Rethinking Suicide” and a leading suicide researcher. At the bottom of his comments there’s a link to the article of which he speaks.
Enjoy!
*****************
From Craig Bryan, LinkedIn – 6/29/2026
We keep trying to predict who will attempt suicide. A 15-year study suggests we’re asking the wrong question.
Researchers followed 2,060 Brazilian children from age 10 into their mid-twenties—one of the longest prospective suicide studies ever conducted outside a high-income country. They measured genetics, perinatal history, family psychiatric illness, childhood adversity, cognition, and clinical symptoms, then tested all of it together against who later attempted suicide.
The result: even with multiple domains of risk factors combined, prediction accuracy stayed modest (AUC 0.665), barely above the ceiling seen across 50 years of suicide research. More sophisticated machine learning models didn’t do any better than simple logistic regression.
Three factors stood out as consistent, actionable, and population-relevant: childhood threat exposure (especially bullying), caregiver history of suicide attempts, and childhood externalizing disorders. Bullying alone accounted for the largest share of preventable risk in the entire study.
The authors’ conclusion is blunt: distal childhood risk factors will likely never predict individual suicide attempts with precision, because suicide is driven by acute, fast-moving processes that a baseline assessment can’t capture. Trying to screen our way to safety has a ceiling. We hit it decades ago.
The better investment may not be sharper prediction. It may be quieter, structural prevention like anti-bullying programs, supporting parents with histories of suicidal behavior, and early identification of behavioral disorders, the kind of intervention that helps a population, whether or not we ever know which child needed it most.
**************************
Here’s the article link: https://lnkd.in/eRWtBiXK
I’m excited about Dr. Bryan’s post not because of the difficulties with prediction (which we’ve long know), but because of the idea of moving upstream toward structural prevention. I also feel this fits really well with what we’re trying to do with CAPE.
Obviously, I love this quotation: “Trying to screen our way to safety has a ceiling. We hit it decades ago.”
Have a great evening!
JSF
How to Grow Wellbeing in Teachers and Schools
I’m at the Office of Public Instruction Summer Institute in Bozeman today (and tomorrow), along with the Pirate and the Pusher. The Summer Institute is an annual four days of training for Montana educators.
Shortly after arriving, two women sitting at a table stared at me, looked away, and then stopped me as I walked by, saying, with enthusiasm, “We just took your class!”
They were, of course, referring to our Happiness for Educators course. Although completely online, I’m presenting in many of the videos, sometimes in my pajamas. We were all excited to meet in person.
They also got to meet Dylan Wright (who plays the role of a pirate in our Happiness for Educators course). I mean, how can you have a Happiness for Educators course without a pirate? They also met Tammy Tolleson Knee, the new and fabulous director of the Phyllis J. Washington Center for the Advancement of Positive Education at the University of Montana and high leverage “Pusher” of all things positive.
Tomorrow will be even more excitement. I have the honor of delivering the morning keynote. I’ll be opening with a make-believe scenario, with me as a candidate for governor. I’ve done this a few times previously during presentations for educators. It’s a method I use for emphasizing the central and foundational role that educators and education play in society.
My platform as a candidate for governor of Montana is education . . . education . . . and education . . . because. . .
The road to a good economy goes through education.
The road to a healthy enviroment goes through education.
The road to a civil society goes through education.
The road to excellence in health care goes through education.
The road to justice goes through education.
I could go on, but I think you get the point. As John Adams, founding father and our 2nd president once said (I’m paraphrasing), “It’s impossible to spend too much money on public education.”
And so, yes, there will be more excitement tomorrow because it doesn’t get much better than spending a day with 400 Montana educators who are dedicated to helping young people become educated citizens.
I’m posting ppts of my two presentations (keynote and workshop) below.
The Secret Retreat

Yesterday, Tammy Tolleson Knee (the new director of the Phyllis J. Washington Center for the Advancement of Positive Education) and I arrived in Kalispell, Montana for a 2+ day retreat with staff from the Nate Chute Foundation (NCF). Their mission: The Nate Chute Foundation supports, educates and empowers our community to promote mental wellness and reduce suicide. You can learn more about NCF’s fabulous work and staff right here: https://www.natechutefoundation.org/
Our retreat is top secret, but I’ll share it here anyway because I don’t like secrets.
Having grown weary with traditional, pathology-oriented approaches to “suicide prevention” we’re working together to create a new curriculum tentatively titled “Strengths-Based Suicide Education for Concerned Adults.” Our plan is to use this new curriculum to replace all the unhelpful and sometimes traumatizing approaches to suicide prevention.
Yes, we have big goals.
Today we’re breaking away from our retreat for a short presentation/consult with Immanuel Living of Kalispell.
In preparation for this short conversation, I pulled out an old slide about a thing called Stress Inoculation Training (thanks Don Meichenbaum!).
The point of SIT is to prepare for stressors or provocations in life that adversely affect us. For example, let’s say that you find ___________ stressful. (You can put anything in the blank. It could be exercise, talking with your boss, going to church, not going to church, speaking in public meetings, etc.). Then you create your own personalized stress inoculation plan.
Meichenbaum’s therapy approach is designed to prep or inoculate us from our usual and predictable stressors. He described three steps: (1) preparation for provocation, (2) coping with the provocative situation, and (3) reflection and self-reinforcement. Here’s a visual, with our stressors and responses organized into 7 dimensions:
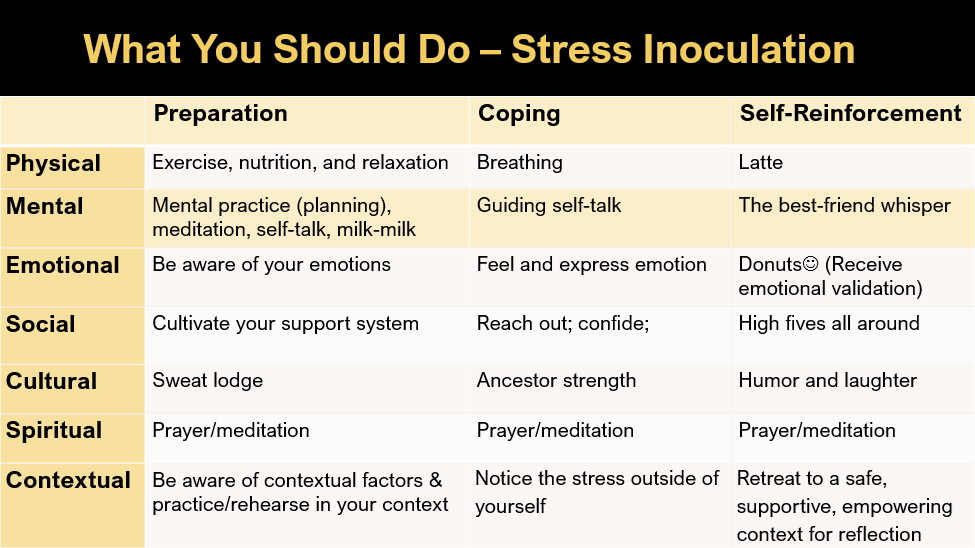
If we all had rational brains and lived in a rational world, SIT would work perfectly for everyone. But like everything, it doesn’t always work. During today’s talk, I’m revealing the secrets of why our best laid plans often fail. Newsflash: it has to do with our quirky brains, which, although amazing, also automatically and regularly take us down into negative thinking rabbit holes.
TBH, IMHO, dipping into a negative thinking rabbit hole every once in a while can be fun, but if your intention was to avoid negative thinking rabbit holes, they’re considerably less fun.
Unfortunately, due to time limits and the need for mystery in marketing, this blog is ending without me sharing the five secrets of why our pesky brains often derail us from our positive intentions. Sorry about that. They’re in the pdf of the ppts linked below, and although you can find them there, it’s much more fun for us to talk about these in person . . . so I hope to see you at a presentation in the future.
Strengths-Based Suicide for Maryland
Good Morning. In a few minutes I’ll be online with the great people of Maryland. Here’s the ppt for the presentation.
Free Online Workshop and CEU Alert: “Strengths-Based Suicide Assessment and Treatment”
Thanks to the generosity of the Maryland Department of Health and the University of Maryland School of Medicine, I’ll be offering a free two-hour online training on Thursday, April 30 from 10am-noon (Eastern time). The flyer (attached below) includes details on the workshop content and a QR code for registering.
04.30.26 Strength – Based Suicide Assessment and Treatment Enhancing Collaborative and Resilience-Oriented Practices Training with Dr. JSFDownload
I hope to see you online on April 30.
2026 ACA World Conference: Strengths-Based Suicide
Along with Kimberly Parrow, this morning I have the privilege of offering a 3-hour workshop at the 2026 ACA Annual Conference.
As always, this is a challenging topic. But in the spirit of a strengths-based approach, it’s important to remember that by engaging in this learning together, we make ourselves stronger, more capable, and more prepared to help clients and students who are feeling suicidal.
Thanks to ACA for the opportunity, to Kim for the help, and for the attendees for being rockstars who are dedicated to helping individuals who are experiencing immense emotional pain and struggling with suicide. You are amazing.
The ppts in pdf:
Ten Things Everyone Should Know about Suicide, Mental Health, and Happiness

Hi All,
My apologies for the late notice, but I’m doing a free, online, one-hour talk tomorrow, 3/4/2026 at 2-3pm Mountain time. Sponsored by the Center for Children, Families, and Workforce Development and MAPP-Net, the talk is titled, “Ten things Everyone Should Know about Suicide, Mental Health, and Happiness.” Here’s the link:
https://www.umt.edu/ccfwd/training/childrenmh_series/
Warning: this is not my most uplifting talk. the first half focuses mostly on the “Wicked Problem” of suicide. The good news is that I do end on Happiness!
Whether you attend or not (it’s free!), thanks for being someone who’s working to make the world a better, kinder, and more eudaimonically happy place.
John
Good Morning Idaho
Here’s the pdf of the ppts for today’s workshop sponsored by Idaho State University.
