This photo is of Lynnel Bullshoe gifting Rita beautiful Indigenous art at a two-day workshop in Browning on the Blackfeet Reservation.
With all the politicizing and media activity around DEI, I think it’s easy to get confused and polarized on DEI issues. Last October, when talking with a friend at a conference in Philly, my friend told a story that I found wonderfully clarifying about DEI. In my previous Theories Preface post, I didn’t include her anecdote–which is one of my favorites–because I didn’t have permission then. But I have permission now, so here’s the missing anecdote:
Recently, a friend of ours told us a story about being asked to deliver a keynote speech for a state school counselor association event. A board member recommended that she “go light on DEI.” Perhaps our friend interpreted that as “You’ve got the green light on DEI,” as the beginning of her speech went something like this:
I was asked to go light on DEI, so I’d like to start by saying, I recently heard someone say that the opposite of diversity is uniformity. The opposite of equity is inequity. The opposite of inclusion is exclusion. And the opposite of anti-racism is racism. I sincerely hope it’s safe to say that as school counselors, none of us want uniformity, inequities, or exclusionary and racist practices.
She went on to remind the audience that we cannot take DEI out of our work, that it is our professional and ethical duty to continuously examine our biases, assumptions, and beliefs, and engage in the ongoing work of self-reflection, learning, and unlearning (J. V. Taylor, personal communication, October 11, 2025).
I love this clear, concise, and beautiful analysis of what is NOT DEI.
Today, Dr. Bossypants (aka Rita) offered me a coauthor opportunity. Thanks Dr. BP!
Problems, like trees, have roots. As Alfred Adler (and many others) would have said, problems are multi-determined, meaning: There’s always more than one root. Most of us agree that the United States has big problems. But what are the roots of our troubles?
One side insists that the roots of our troubles include unworthy and illegal immigrants, burdening the rich with taxes, satanic trans folk, welfare fakers, and bleeding hearts. The media picks up this messaging, repeating these highly questionable theories until they sink into our psyches as if they were true.
But we are being played.
As they said back in the Watergate era, follow the money.
The rare transgender athlete is not to blame for your low wages or the price of food and shelter. Tending to the disabled and disadvantaged is not breaking the bank. Social Security makes us a strong, compassionate society—providing for all of us as we age. Social Security isn’t going broke. It’s being dismantled and privatized so the wealthy benefit.
We’re chopping off our noses to spite our faces. USAID greatly contributed to the health of the poor, the planet, and developing societies trying to recover, survive, and grow. NPR and PBS cost about $1.50 per person per year. Although their coverage has been leaning right, they work toward being objective, balanced, and accurate. A free press is at the heart of democracy.
Hiding the contributions of people of color from American history involves rewriting reality. What might be the purpose of excluding honorable actions and voices of diverse individuals and groups from our history? There’s an African proverb: “Until lions have their historians, tales of the hunt shall always glorify the hunter.” Preserving real history doesn’t make us less safe. Massive salaries, bonuses, and advantages given to those mismanaging and/or dismantling our social and financial safety nets is a real danger.
Billionaires have lied so well for so long that many Americans blame poor people and the middle class for government waste and fraud. As everyone admits, government waste and fraud exist, and there are effective strategies for minimizing waste and fraud. One billionaire strategy is this: Get the American people to blame each other for their financial woes. Then, through their tax loopholes, billionaires walk right into the henhouse and steal the country’s eggs.
Most billionaires don’t become billionaires because of their compassion and generosity. They’re billionaires because of miners, farmers, mill workers, steelmakers, refinery workers, teachers, servers, nurses, doctors, social workers, inventors, and small businesspeople: THESE are the people who make becoming a billionaire possible.
Balanced budgets are possible. Giving billionaires MORE money will not balance the budget. Taxing them more will. A graduated income tax is not the same thing as socialism. Anyone who tells you that taxing the rich and providing a social safety net is socialism or communism either (a) wants YOUR money, (b) is lying, or (c) is ignorant.
Socialism is a political and economic theory advocating that the means of production, distribution of goods, and trade/exchange be owned by the collective. Taxing the wealthy in a proportionate manner is not the same as having the collective or the government take over ownership of their businesses. In a capitalist system, taxes and government regulation function to reduce power imbalance, abuse of the poor by the wealthy, and the development of social safety nets and public health systems that benefit the whole.
The ugly fights we’re in now were started purposefully and fueled by lies, phony moral outrage, purchased bots and paid “news” outlets. We’ve been duped into “culture wars.” As if a gay marriage is why you aren’t paid fairly. As if God needs guns to defend holiness. As if basic health care for everyone will cost more than our broken system. As if we cannot share bathrooms. We share bathrooms all the time in our homes, while camping, at outdoor sporting events (think porta potties). Our economic and social problems are NOT ABOUT BATHROOMS.
We would say “wake up,” but the billionaires have cleverly stolen that concept. They want us asleep. They want us less educated, less compassionate, and more frightened.
Those in power twist science, scripture, economics, virtue, common sense, and the idea of community. But they can’t take your soul; they can’t eliminate your deep awareness of right and wrong. Only you can do that.
Ask yourselves:
If climate change caused by humans is wrong, why not clean things up anyway? Powerful people can say “drill baby drill” and it sounds aggressively American, but really, who’s pro-pollution? Denying climate change will cost us our planet.
All religions, including Christianity, advocate for taking care of the poor. Yes, it costs a few shekels. But do we want the alternative? Shall we harden our hearts and let others suffer and die?
If you believe YOU should have control over your own body and your own sexual decisions, maybe YOU can let others own their bodies and make their own choices as well?
Science is not a simplistic fact-finding mission. Science is a disciplined process of inquiry. Scientific knowledge has saved millions of lives. Funding science is about progress and having a higher quality of living. Superstition, politicizing, and irrational attacks on science is regressive, ignorant, and dangerous.
Do you think the Creator expects YOU to force your version of morality onto others? Should you enforce thou shalt not kill with weapons? Aren’t you busy enough just finding the time and resources to love your neighbor? Care for the poor? Offer your coat to anyone who needs it? It takes a lifetime to remove the log in your eye, so you can see well enough to help someone with a splinter? Isn’t God, by definition, omnipotent? We should all stop confusing our will, our interests, and our greed, with God’s will.
We need the rule of law. When people in power disregard and disparage the courts, they’re not acting for the common good. If we lose the rule of law, we’ll be ruled by outlaws.
Over our long history, humans have been conned, cheated, manipulated, and enslaved many times by the rich, powerful, and depraved. Trusting billionaires and others who are energized by the pursuit of power, greed, and revenge does not end well.
Tomorrow morning, three counseling interns and I will hit the road for Ronan, where we’ll spend the day with the staff of CSKT Tribal Health. We are honored and humbled to engage in a conversation about how to make the usual medical model approach to suicide be more culturally sensitive and explicitly collaborative.
Why Do We Need a Strengths-Based Approach to Suicide Assessment and Treatment?
Imagine this: You’re living in a world that seems like it would just as soon forget you exist. Maybe your skin color is different than the dominant people who hold power. Maybe you have a disability. Whatever the case, the message you hear from the culture is that you’re not important and not worthy. You feel oppressed, marginalized, unsupported, and as if much of society would just as soon have you become invisible or go away.
In response, you intermittently feel depressed and suicidal. Then, when you enter the office of a health or mental health professional, the professional asks you about depression and suicide. Even if the professional is well-intended, judgment leaks through. If you admit to feeling depressed and having suicidal thoughts, you’ll get a diagnosis that implies you’re to blame for having depressing and suicidal thoughts.
The medical model overfocuses on trying to determine: “Are you suicidal?” The medical model is also based on the assumption that the presence of suicidality indicates there’s something seriously wrong with you. But if we’re working with someone who has been or is currently being marginalized, a rational response from the patient might be:
“As it turns out, I’ve internalized systemic and intergenerational racism, sexism, ableism, and other dehumanizing messages from society. I’ve been devalued for so long and so often that now, I’ve internalized societal messages: I devalue myself and wonder if life is worth living. And now, you’re blaming me with a label that implies I’m the problem!”
No wonder most people who are feeling suicidal don’t bother telling their health professionals.
When I think of this preceding scenario, I want to add profanity into my response, so I can adequately convey that it’s completely unjust to BLAME patients for absorbing repeated negative messages about people who look like or sound like or act like them. WTH else do you think should happen?
This is why we need to integrate strengths-based principles into traditional suicide assessment and prevention models. Of course, we shouldn’t use strengths-based ideas in ways that are toxically positive. We ALWAYS need to start by coming alongside and feeling with our patients and clients. As it turns out, if we do a good job of coming alongside patients/clients who are in emotional pain, natural opportunities for focus on strengths and resources, including cultural, racial, sexual, and other identities that give the person meaning.
I’m reminded of an interview I did with an Alaskan Native person from the Yupik tribe. She talked at length about her depression, about feeling like a zombie, and past and current suicidal thoughts. Eventually, I inquired: “What’s happening when you’re not having thoughts about suicide?” She seemed surprised. Then she said, “I’d be singing or writing poetry.” I instantly had a sense that expressing herself held meaning for her. In particular, her singing Native songs and contemporary pop songs became important in our collaborative efforts to build her a safety plan.
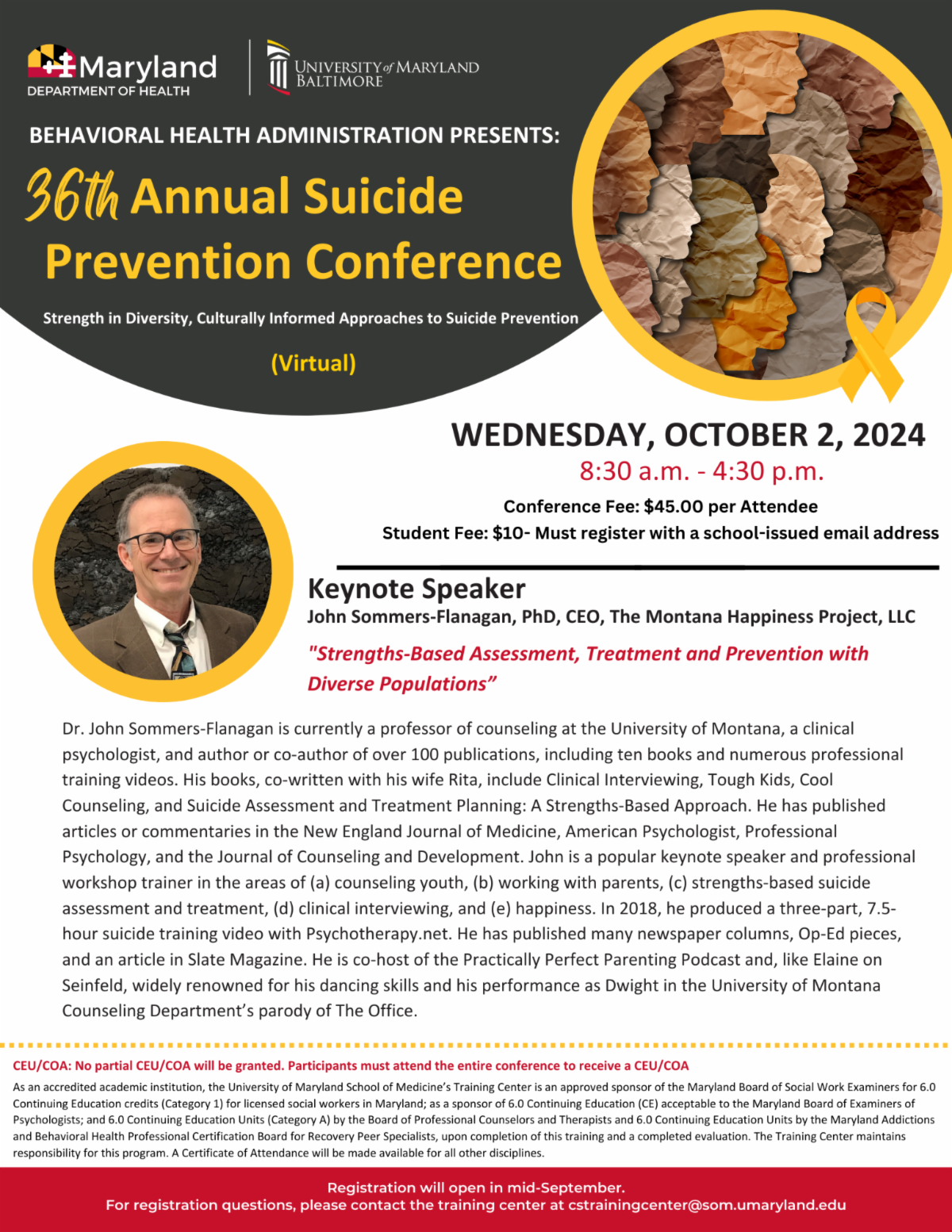
This coming Wednesday morning I have the honor of presenting as the keynote speaker for the Maryland Department of Health 36th Annual Suicide Prevention Conference. During this keynote, I’ll share more ideas about why a strengths-based model is a good fit when working with diverse clients who are experiencing suicidal thoughts and impulses.
With all that said, here’s the title and abstract of my upcoming presentation.
Strengths-Based Assessment, Treatment, and Prevention with Diverse Populations
Traditional suicide assessment tends to be a top-down information-gathering process wherein healthcare or prevention professionals use questionnaires and clinical interviews to determine patient or client suicide risk. This approach may not be the best fit for people from populations with historical trauma, or for people who continue to experience oppression or marginalization. In this presentation, John Sommers-Flanagan will review principles of a strengths-based approach to suicide prevention, assessment, and treatment. He will also discuss how to be more sensitive, empowering, collaborative, and how to leverage cultural strengths when working with people who are potentially suicidal. You will learn at least three practical strengths-based strategies for initiating conversations about suicide, conducting culturally-sensitive assessments, and implementing suicide interventions—that you can immediately use in your prevention work.
I’m continuing with the theme of featuring diverse identities from the Clinical Interviewing (7th edition) textbook with a case example written by Dr. Umit Arslan. Dr. Arslan is writing about his experience as an international graduate student in counseling, when he was at the University of Montana. Currently, he’s a faculty member at the University of Nebraska-Kearney.
The photo is from when I visited him in Istanbul in January, 2023.
Enjoy!
As you’ll see below, Umit’s experience was unique. Given his Turkish heritage and cultural background, he needed to reflect and engage in a self-awareness process to experiment with finding a better way to introduce himself to clients. What I love most about this essay is Umit’s authentic description of his own experience. His answer to a better way to introduce himself won’t be the right answer for everyone. But his process is open and admirable.
CASE EXAMPLE 2.2: BEING A COUNSELOR FIRST . . . AND TURKISH SECOND, WORKED BETTER THAN BEING TURKISH FIRST . . . AND A COUNSELOR SECOND
Finding the right words and ways to introduce yourself is important. In this essay, Ümüt Arslan, Ph.D., an associate professor of counseling at İzmir Democracy University (Turkey), writes about challenges he faced as an international doctoral student in counseling at the University of Montana. Put yourself in Dr. Arslan’s shoes as he discovers (for him) a better way of introducing himself.
While pursuing my doctoral degree in the U.S., my supervisor and I discussed how to share my cultural identity and accent to clients. When I shared, my clients were not only interested in my appearance and accent, but also about my diet, coffee preferences, job, and of course, about my native country, Turkey. But they were reluctant to talk about themselves.
Clients assumed I was Muslim and against alcohol. Their assumptions were especially challenging because they were inaccurate. I was not religious, and like many Americans, I enjoyed having a beer after work. I wanted to challenge clients’ assumptions about my identity, but worried about countertransference and focusing too much on myself.
One cisgender female client came for an intake interview. She saw me, grabbed her bag (almost the size of a camping tent), and put it on her knees. I couldn’t see her face. I told her she could put the bag down if she wanted to. She declined.
When I re-watched this and other sessions, the striking thing was that my clients (mostly White) appeared stressed at the sight of me, a bearded Turkish man with dark skin. They didn’t even talk about the problems they had written on their intake form. My identity as a Turkish man overshadowed everything else. I needed a path forward.
In class, my supervisor discussed alternative ways to open sessions. I tried asking clients: “If you were the counselor today, what question would you ask yourself?” Clients suddenly engaged with me, giving deep and enthusiastic answers to their own questions. I stopped opening sessions by emphasizing cultural differences. Instead, I focused on my counselor identity, saying: “I completed my master’s degree and am currently a doctoral student. What do you think is the best question for me to ask you for us to have a good start here today?”The message, “I am here with my counselor identity” instead of “I’m a Turkish man in the U.S., and desperate to explain my culture to you,” had an amazing effect. Using a less cultural opening was more culturally sensitive. Clients could naturally introduce their own cultural identities, with fewer assumptions about me. Although I could still talk about culture, emphasizing my counselor identity enabled me to focus on counseling goals, the therapeutic relationship, and evidence-based counseling interventions.
To continue with my plan to feature culturally diverse case examples from the latest edition of Clinical Interviewing, the following excerpt is from Chapter One and focuses on cultural self-awareness. In particular, I LOVE the quotation on intersectionality from Kimberlé Crenshaw.
Cultural Self-Awareness
Those who have power appear to have no culture, whereas those without power are seen as cultural beings, or “ethnic.” (Fontes, 2008, p. 25)
Culture and self-awareness interface in many ways. As Fontes (2008) implied, individuals from dominant cultures tend to be unaware of and often resistant to becoming aware of their invisible and unearned culturally-based advantages (Sue et al., 2020). In the U.S., these “unearned assets” are often referred to as privilege in general, and White privilege in particular (McIntosh, 1998).
Privilege and oppression are best understood in the context of intersectionality. Intersectionality is the idea that overlapping or intersecting social identities within individuals create whole persons that are different from the sum of their parts (Crenshaw, 1989). Social identities that intersect include, but are not limited to: Gender, sexual orientation, sexual identity, race, ethnicity, religion, nationality, mental disorder, physical disability/illness, citizenship, and social class (Hays, 2022). Understanding multiple social identities helps clinicians understand how feelings of oppression can multiply, be activated under distinct circumstances, and be moderated under other circumstances.
Kimberlé Crenshaw (1989, 1991) introduced intersectionality as a lens to facilitate cultural awareness and understanding, but ideas about intersectionality date back at least to Black female abolitionists. In the 1860s, Sojourner Truth articulated Black women’s simultaneous oppression through classism, racism, and sexism (aka “Triple oppression”; Boyce Davies, 2008). Thirty years after she defined intersectionality, Time Magazine asked Crenshaw, “You introduced intersectionality more than 30 years ago. How do you explain what it means today?” (Steinmetz, 2020). She said,
These days, I start with what it’s not, because there has been distortion. It’s not identity politics on steroids. It is not a mechanism to turn white men into the new pariahs. It’s basically a lens, a prism, for seeing the way in which various forms of inequality often operate together and exacerbate each other. We tend to talk about race inequality as separate from inequality based on gender, class, sexuality or immigrant status. What’s often missing is how some people are subject to all of these, and the experience is not just the sum of its parts.
Through the lens of intersectionality, we can develop nuanced ways to have empathy for clients. For example, sometimes clients simultaneously feel privilege and oppression. Thinking and feeling from an intersectional frame can help clinicians be more prepared to view the world from clients’ perspectives (see Case Example 1.2).
CASE EXAMPLE 1.2: EMPATHY FIRST
Maya, an international student of color was in her first practicum. As was her routine, when introducing herself, she acknowledged her accent, her country of origin, along with her eagerness to be of assistance. Her client, a cisgender male university student, was initially polite, but quickly shifted the conversation to his feelings about White privilege, becoming somewhat agitated in the process. He said, “One thing I think you should know that I don’t believe in that White privilege thing. I just came from a class where that’s all everyone was talking about. I know I’m white, but I didn’t get any privilege. I grew up in a trailer park in West Texas. We were what they call ‘White trash.’ Nobody I grew up with had any privilege. We had poverty, abuse, alcoholism, meth, and government bullshit.”
Maya stayed calm. Even though she was activated by her client’s disclosure and was taking some of what he said personally, she focused on empathy first. She also remembered intersectionality and how common it could be for people to have multiple social identities. She said, “I hear you saying that the White privilege concept really doesn’t fit for you. Being in your very last class before coming here made you realize even more that it doesn’t fit. The idea of trying to make it fit feels annoying.”
Maya’s client simply said, “Damn right,” and continued ranting about White privilege, White fragility, and what he viewed as the politically correct environment at the university. As she continued listening and tried feeling along with him, she was able to see glimpses of his personal perspective. Not surprisingly, Maya’s client had social problems related to his tendency to be angry and abrasive. Eventually, after several sessions, they were able to begin talking about what was underneath his agitated emotional response to multicultural ideas and how his tendency to lead with his anger when in conversations with others might be contributing to him feeling even more isolated and different than everyone else. In the end, the client thanked Maya for “being patient with this dumb ass White boy” and helping him learn to be more aware, softer, and less reactive to triggering cultural conversations.
This case illustrates the importance of intersectionality as a concept that can facilitate counselor and client awareness, while also enhancing empathy. Although Maya’s client may have had even worse oppressive experiences had he been a person of color, he was neither interested nor ready to hear that message (Quarles & Bozarth, 2022). Instead, Maya used her knowledge of intersectionality to have empathy with the part of her client’s social identity that had experienced oppression.
Developing cultural self-awareness is difficult. One way of expressing this is to note, “We don’t know what we don’t know.” When someone tries to help us see and understand something about ourselves that’s outside our awareness, it’s easy to feel defensive. Despite the challenges, we encourage you to be as eager for change and growth as possible, and offer three recommendations:
Be open to exploring your own cultural identity. Gaining greater awareness of your ethnicity is useful.
If you’re from the dominant culture, be open to exploring your privilege (e.g., White privilege, wealth privilege, health privilege) as well as hidden ways that you might judge or have bias toward diverse groups and individuals (e.g., transgender, disabled).
If you’re outside the dominant culture, be open to discovering ways to have empathy not only for members within your group, but also for other diversities and for the struggles that dominant cultural group members might have as they navigate challenges of increasing cultural awareness. Engaging in mutual empathy is a cornerstone of relational cultural psychotherapy (Gómez, 2020).
For the next several weeks I’ll be sharing from our almost new 7th edition of Clinical Interviewing.
One of our goals for the 7th edition of Clinical Interviewing is to move toward greater representation of different ethnic/cultural/sexual identities. We want all potential counseling, psychology, and social work students to be able to identify with counseling, psychology, and social work professionals. To accomplish this goal, we added greater representation by broadening our usual chapter content, as well as including case examples contributed by professionals with diverse identities.
Here’s an excerpt from Chapter 1 on culture-specific expertise
******************************************
Culture-Specific Expertise
Culture-specific expertise speaks to the need for clinicians to learn skills for working effectively with diverse populations. For example, learning the attitudes and skills associated with affirmative therapy is important for clinicians working with diverse sexualities, including lesbian, gay, bisexual, transgender, queer/questioning (sexual or gender identity), intersex, and asexual/aromantic/agender (LGBTQIA+) clients (Heck et al., 2013). Similarly, integrating skills for talking about spiritual constructs into your work with African American, Latinx, Indigenous, and traditionally religious clients is often essential (Mandelkow et al., 2021; Sandage & Strawn, 2022).
Stanley Sue (1998, 2006) described two general skills for working with diverse cultures: (a) scientific mindedness and (b) dynamic sizing.
Scientific mindedness involves forming and testing hypotheses about client culture, rather than coming to premature conclusions. Although many human experiences are universal, it’s risky to assume you know the underlying meaning of your clients’ behavior, especially minoritized clients. As Case Example 1.3 illustrates, culturally sensitive clinicians avoid stereotypic generalizations.
Dynamic sizing is a complex multicultural concept that guides clinicians on when they should and should not generalize based on an individual client’s belonging to a specific cultural group. For example, filial piety is a value associated with certain Asian families and cultures (Ge, 2021). Filial piety involves the honoring and caring for one’s parents and ancestors. However, it would be naïve to assume that all Asian people believe in or have their lives affected by this particular value; making such an assumption can inaccurately influence your expectations of client behavior. At the same time, you would be remiss if you were uninformed about the power of filial piety in some families and the possibility that it might play a large role in relationship and career decisions in many Asians’ lives. When clinicians use dynamic sizing appropriately, they remain open to significant cultural influences, but they minimize the pitfalls of stereotyping clients.
Another facet of dynamic sizing involves therapists’ knowing when to generalize their own experiences to their clients. S. Sue (2006) explained that it’s possible for clinicians who have experienced discrimination and prejudice to use their experiences to more fully understand the discrimination-related struggles of clients. However, having had experiences similar to a client may cause you to project your own thoughts and feelings onto that client—instead of drawing out the client’s emotions and showing empathy. Dynamic sizing requires that you know and understand and not know and not understand at the same time. Not knowing—or at least not presuming you know—is essential to interviewer-client collaboration.
CASE EXAMPLE 1.3: NOT AT HOME ANYWHERE
In this case, Devika Dibya Choudhuri, Ph.D., LPC (CT/MI), a self-described Buddhist, South Asian, cisfemale, middle-aged, middle-class, Queer, disabled counselor and professor at Eastern Michigan University, illustrates sophisticated cultural-specific expertise in cross-cultural work with a bi-cultural college student. Dr. Choudhuri uses self-disclosure, researches her client’s culture, and integrates culturally meaningful symbols into her sessions. Imagine how you can aspire to be like Dr. Choudhuri.
Darla, a 19-year-old Ghanian-American cisfemale college student, felt something was wrong with her. Her mother was from Ghana, while her father, with whom she had little contact, was generationally African American. She was halting in the first session, trying to decide whether she could trust me, and talking about her recent visit to Accra where her mother’s family lived. I said, “I know when I go to India, I’m American, and when I’m here, I’m Indian. Is it a bit like that for you?” She emphatically replied, “Yes! I’m not at home anywhere!” “Or,” I returned, “almost at home everywhere, like the rest of us global nomads.” She laughed, then spoke far more comfortably about her friends and boyfriend. I had, in that brief exchange, told Darla very important things about me. I self-disclosed casually about my ethnicity and international navigation, normalized her sense of homelessness, while reframing it to join a new group identity.
After having done some research, I asked Darla if her Ghanian kin were the majority Akan or a minority group. She said they were minority. I reflected on whether she might have picked up a sense of marginalization, not just from being Black in America, but also from being minority in Ghana. This became a deep and intense conversation. She reflected on how her American status in Ghana protected her from discrimination, but also alienated her from her cousins.
Another use of culture as intervention came when I brought in Adinkra (visual pictograph meaning saturated symbols originating in Ghana) for her use. Darla chose four to represent her aspirations, and then designed ways to use them in her daily life, incorporating her cultural roots into her present. One of them, Sankofa, is a symbol of the wisdom of learning from the past to build for the future; expressed in the proverb, “it is not taboo to go back for what you left behind.” Feeling grounded in multiple cultures, and being able to navigate from one context to another with her whole and complex self, rather than fragmenting, led her to see she wasn’t “wrong.” Sometimes the spaces were too limited; it was ok to fit and not fit, just as leftover food on a Ghanian table represented abundance.
[End of Case Example 1.3]
******************************************
As always, feel free to share your thoughts on and reactions to this content. We’re always looking for practical feedback that will help us continue to become better learners and teachers.
Early this morning, I had a chance to Zoom in and present a workshop for Saint Michael’s College in Vermont. This was probably a good thing, because they had more than their share of snow to deal with. I got to be in Vermont virtually from beautiful Missoula Montana, where we’ve had spring most of winter. I wish we could borrow a few feet of that Vermont snow to get us up to something close to normal.
But my point is to share my ppts from this morning, and not talk about the weather. I had a great two hours with the Saint Michael’s professionals . . . as they posed excellent and nuanced questions and made insightful comments. Here’s a link to the ppts:
Last week I was dancing and singing in India at my nephew’s wedding. This week I’m jet-lagged in Missoula. But the afterglow continues.
Being at a wedding, it was hard not to think of my mother. She loved weddings and always wished for everyone to find love.
My sisters had similar thoughts. We reminisced and projected my mother into the scene of my nephew marrying an Asian Indian woman in a Hindu ceremony. We wished she could pop back into the world and join in.
Mostly, my mother was shy and insecure. She didn’t learn to drive until age 34. I often wished she had more confidence.
But there was one place where my mom found her voice, early and often. For mysterious and obvious reasons, she became anti-racist in the 1950s, before anti-racism was a thing. She delighted in visits from my father’s Japanese friend, Carl Tanaka. When a Black family moved onto our all-White dead-end suburban street, she was the first to greet them with welcome gifts. She then sat my sisters and I down, and told us with piercing clarity that we would ALWAYS treat every member of that family with nothing but respect and kindness. They quickly became our friends. I have great memories of hanging out with my friend Darrell, who was the closest to me in age and in school.
What I didn’t understand about my mom’s anti-racism—until last week—was that she also had a solution. My sisters told me that my mother’s favorite solution to all that ails the world was inter-racial, inter-cultural, and inter-religion marriage. Of course, I’m not naïve enough to think that any single strategy could solve racism, but last week, during a three-day Hindu marriage ceremony, I returned home transformed and preoccupied with the idea that we can and should love one another.
The internet tells me that love one another has Christian Biblical origins . . . and more. Here’s an excerpt from a site that discusses “love of neighbor” in Hinduism.
Love of the neighbor or the “other soul” is a fundamental requirement for a functioning Hindu who aspires for final liberation from this world. Any injury or insult inflicted upon the other soul is ultimately injury inflicted on oneself—or worse still, the higher being. Neighborly love is integral for one’s social existence in this world. The Anusana Parva (113:8) in Mahabharata encapsulates this wisdom and dictates that one should be unselfish and not behave toward others in a way that is disagreeable to oneself. [From: http://what-when-how.com/love-in-world-religions/love-of-neighbor-in-hinduism/]
The facts were that Stephen Klein married Sahana Kumar last week, in a beautiful coastal setting just south of Chennai, India.
In a marvelous stroke of luck, I happen to be Gayle Klein’s brother and Stephen’s Uncle John. Along with the dancing singing (which I may have overdone), I was completely taken by the intercultural love and acceptance. The Kumar family welcomed Stephen and all of us to be with them not only in the celebration, but in relationship. At the Sangeet, we were invited to dance a Bollywood and a Hollywood dance. We were terrible AND we were completely accepted. To be immersed in another culture, to learn about Hinduism, to experience glimpses of the Southern Indian cultural ways of being . . . was AMAZING.
In love and in relationship, we often fall short. It’s hard to love our politically different family members. It’s hard to love when we feel annoyed. Sometimes, as I heard the famous Julie and John Gottman say, it’s even hard to find the time and timing to love our romantic partners. But love is big and, thanks to my sisters and Stephen, Sahana, and the Kumars, I understand love a little better this week. The intent to love people who are different than us; the invitation to be in relationship across cultures and generations; the desire to be as loving as we can be . . . those are the ways of being my mom might be shouting from the heavens.
These days mostly we tend to orient toward the culturally specific, and that’s a good thing. Much of intersectionality, cultural competency, and cultural humility is all about drilling down into unique and valuable cultural and individual perspectives.
But these are also the days of Both-And.
In contrast to cultural specificity, some theorists—I’m thinking of William Glasser right now—were more known for their emphasis on cultural universality. Glasser contended that his five basic human needs were culturally universal; those needs included: Survival, belonging, power (recognition), freedom, and fun.
Although Glasser’s ideas may (or may not) have universal punch, he’s a white guy, and pushing universality from positions of white privilege are, at this particular point in history, worth questioning. That’s why I was happy to find an indigenous voice emphasizing universal ideas.
I came across a quotation from a Lakota elder, James Clairmont; he was discussing the concept of resilience, from his particular linguistic perspective:
The closest translation of “resilience” is a sacred word that means “resistance” . . . resisting bad thoughts, bad behaviors. We accept what life gives us, good and bad, as gifts from the Creator. We try to get through hard times, stressful times, with a good heart. The gift [of adversity] is the lesson we learn from overcoming it.
Clairmont’s description of “the sacred word that means resilience” are strikingly similar to several contemporary ideas in counseling and psychotherapy practice.
“Resisting bad thoughts, bad behaviors” is closely linked to CBT
“We accept what life gives us, good and bad, as gifts from the Creator” fits well with mindfulness
“We try to get through hard times, stressful times, with a good heart” is consistent with optimism concepts in positive psychology
“The gift [of adversity] is the lesson we learn from overcoming it” and this is a great paraphrase of Bandura’s feedback and feed-forward ideas
In these days of cultural specificity, it makes sense to work from both perspectives. We need to recognize and value our unique differences, while simultaneously noticing our similarities and areas of convergence. Clairmont’s perspectives on resilience make me want to learn more about Lakota ideas, both how they’re similar and different from my own cultural and educational experiences.
The place to click if you want to learn about psychotherapy, counseling, or whatever John SF is thinking about.