Below, I’ve a pasted LinkedIn post from Dr. Craig Bryan, author of “Rethinking Suicide” and a leading suicide researcher. At the bottom of his comments there’s a link to the article of which he speaks.
Enjoy!
*****************
From Craig Bryan, LinkedIn – 6/29/2026
We keep trying to predict who will attempt suicide. A 15-year study suggests we’re asking the wrong question.
Researchers followed 2,060 Brazilian children from age 10 into their mid-twenties—one of the longest prospective suicide studies ever conducted outside a high-income country. They measured genetics, perinatal history, family psychiatric illness, childhood adversity, cognition, and clinical symptoms, then tested all of it together against who later attempted suicide.
The result: even with multiple domains of risk factors combined, prediction accuracy stayed modest (AUC 0.665), barely above the ceiling seen across 50 years of suicide research. More sophisticated machine learning models didn’t do any better than simple logistic regression.
Three factors stood out as consistent, actionable, and population-relevant: childhood threat exposure (especially bullying), caregiver history of suicide attempts, and childhood externalizing disorders. Bullying alone accounted for the largest share of preventable risk in the entire study.
The authors’ conclusion is blunt: distal childhood risk factors will likely never predict individual suicide attempts with precision, because suicide is driven by acute, fast-moving processes that a baseline assessment can’t capture. Trying to screen our way to safety has a ceiling. We hit it decades ago.
The better investment may not be sharper prediction. It may be quieter, structural prevention like anti-bullying programs, supporting parents with histories of suicidal behavior, and early identification of behavioral disorders, the kind of intervention that helps a population, whether or not we ever know which child needed it most.
I’m excited about Dr. Bryan’s post not because of the difficulties with prediction (which we’ve long know), but because of the idea of moving upstream toward structural prevention. I also feel this fits really well with what we’re trying to do with CAPE.
Obviously, I love this quotation: “Trying to screen our way to safety has a ceiling. We hit it decades ago.”
Thanks to the generosity of the Maryland Department of Health and the University of Maryland School of Medicine, I’ll be offering a free two-hour online training on Thursday, April 30 from 10am-noon (Eastern time). The flyer (attached below) includes details on the workshop content and a QR code for registering.
As a senior in high school, I had a chance to say a few words at the annual football awards banquet. Apparently, my stammering and stuttering through two whole minutes were so inspiring that afterward, an assistant coach took me aside and offered seven words of feedback, “You need to take a speech class.”
His words sunk in. I was a terrible and inarticulate speaker. But did I take his advice? Nope. I was too scared to even try to get better at public speaking.
Fast forward 51 years. Now I speak all the time. In one of my most recent speaking gigs, David Shepard and Erica Liebman had me on their very cool podcast called, “Therapy with Men and Boys.”
On the podcast, we talked about men and boys and therapy and suicide. We talked so much they made my appearance into two episodes. And David, whose work I respect a ton, told me, “Your comfort in front of a mic is really impressive. I can imagine how much your students liked your classes in your teaching days.”
Thanks David! What a difference 51 years makes.
I share this story because things change with time. . .and I’m hoping (in the sociocultural-political realms) that time will change some things (for the better).
If you’re interested in therapy in general and therapy with men and boys in particular, I’m sharing links to part 1 and 2 of the podcast; they’re about 35 minutes each.
My apologies for the late notice, but I’m doing a free, online, one-hour talk tomorrow, 3/4/2026 at 2-3pm Mountain time. Sponsored by the Center for Children, Families, and Workforce Development and MAPP-Net, the talk is titled, “Ten things Everyone Should Know about Suicide, Mental Health, and Happiness.” Here’s the link:
Warning: this is not my most uplifting talk. the first half focuses mostly on the “Wicked Problem” of suicide. The good news is that I do end on Happiness!
Whether you attend or not (it’s free!), thanks for being someone who’s working to make the world a better, kinder, and more eudaimonically happy place.
Today, Tammy Tolleson Knee and completed day 1 of a 2-day course on Strengths-Based Suicide Assessment and Interventions in Schools at the Buffalo Hide Academy of Browning Public Schools on the Blackfeet Reservation. We are beyond happy for this opportunity. It’s the first time for Tammy and I to present together (for two days!). As frosting on the presentation cake, Rita is here with us, watching, listening, heckling, and guiding.
In case you haven’t heard, Browning Public Schools and their staff have already started integrating strengths-based suicide prevention work into their programming. Two of our former University of Montana school counseling graduates, Sienna and Charlie Speicher are at the center of this work. Sienna and Charlie have already taught strengths-based courses through Blackfeet Community College, and they founded the Firekeeper Alliance. Here’s the Firekeeper Alliance Mission Statement:
Our mission is to cultivate resources, attention, and awareness to ultimately transform perspectives regarding suicidal distress in Indian Country and to help reduce suicide rates in our communities. We believe that mainstream and current approaches of suicide assessment and intervention struggle to meet the unique needs of Tribal populations. The Firekeeper Alliance promotes a different set of strengths-based, decolonized ideals around suicidal behavior. We believe that systemic and cultural shifts in the clinical community are necessary to truly make a positive change.
The Firekeeper Alliance also focuses on several areas, including offering strengths-based approaches to counseling, as in the following:
Offer individual and group counseling sessions utilizing evidence-based therapies which are effective in addressing suicidality.
Promote assessment techniques and interventions that elicit protective factors and a resilient spirit.
Administer assessment instruments that screen for strengths, character assets, and benevolent experience to depathologize suicidal distress.
Advocate for strengths based assessment and intervention approaches to be used in conjunction with cultural healing mechanisms.
Back to our training. . .here are the ppts that Tammy and I developed. There are SO MANY, but then again, we’re covering two whole days!
In closing, I want to give a big shout-out to Browning Public Schools (BPS) for collaborating with us (the Center for the Advancement of Positive Education; aka CAPE) to bring this training to Browning. Not only do we have a dozen or so school counselors in the room, we’ve also got a dozen or so administrative staff, including principals and the BPS superintendent. We had a blast today and are looking forward to more meaningful fun tomorrow!
Yesterday I was in Arkansas with the Arkansas Psychological Association talking about Strengths-based Suicide Assessment. And today I’m in Philly, along with Dr. Umit Arslan (and missing Tammy Tolleson-Knee) talking about it again–at the Association of Counselor Education and Supervision conference.
Unfortunately, Tammy’s efforts to get here were foiled by a particular airline fiasco, but we’re carrying on! We miss you Tammy!
All too often on this blog I’m writing about what I’m doing and I’m thinking. I suppose that’s just fine, after all, it’s my blog. But, as many people have said before me and better than I can, “Other people matter” and seeing the light (or the divine) in others is among the most meaningful experiences we can have.
One light I’ve been seeing lately is the strengths-based suicide prevention work that the Firekeeper Alliance (a non-profit org) is doing on the Blackfeet Reservation in Northern Montana. In July, they had a “suicide prevention” heavy metal concert called Fire in the Mountains, complete with amazing metal bands and equally amazing panels, discussions, and speakers. If you’re interested in creative approaches to well-being, you really should check them out.
This past Thursday, Charlie Speicher, architect of the Firekeeper Alliance and Director of the Buffalo Hide Academy in Browning, shared one of their Suicide Prevention Month activities. The idea is simple: Feature the beauty and strengths of the reservation and its people. The product: A 12-minute video that focuses on what gives the Blackfeet people hope. The video captures the faces, sentiments, and emotions in response to “What gives you hope?” Here’s the link on Youtube:
All too often, people think and share information about the challenges of reservation life. This video shares hope, beauty, and potential.
With your help, I hope this video travels far and wide. Please share. At the very least, it should get all over Montana media. And, just in case anyone has the right connections, I think it’s a great fit for virtually any national media outlet that wants to shift toward a positive narrative in Indian Country.
Thanks for reading . . . and for seeing the light (and fire) in others.
Last Friday night (or Saturday morning in South Korea), I had the honor and privilege of spending three hours online with 45 South Korean therapists. We were talking, of course, about strengths-based suicide assessment and treatment. Given my limited Korean language skills (is it accurate to say my language skills are limited if I can’t say or comprehend ANYTHING in Korean?), I had a translator. Although I couldn’t tell anything about the translation accuracy, my distinct impression was that she was absolutely amazing.
I had a friend ask how I happened to get invited to present to Korean therapists. My main response is that I believe the time is right (aka Zeitgeist) for greater integration of the strengths-based approach into traditional suicide assessment and treatment. The person who recruited me was Dr. Julia Park, another absolutely amazing, kind, and competent South Korean person, who also happens to hold an Adlerian theoretical orientation. Thanks Julia!
Just for fun, I wish I had my Korean translated ppts to share here. They’re unavailable, and so instead I’m sharing an excerpt from Chapter 10 (Suicide Assessment Interviewing) of our Clinical Interviewing (2024) textbook. The section I’m featuring is the part where we review issues and procedures around suicide risk categorization and decision-making.
You may already know that some of the latest thinking on suicide risk assessment is that we should not use instruments like the Columbia to categorize risk. You also may know that not only am I a believer in this latest thinking, I can be wildly critical of efforts to categorize suicide risk. . . so much so that I often end up using profanity in my professional presentations. Of course, because the context is a professional presentation, I only use the highly professional versions of profanity.
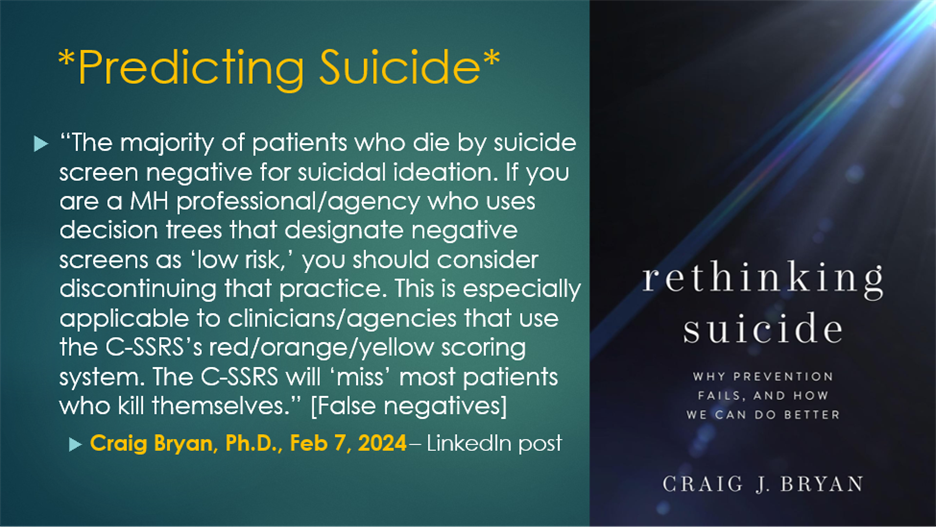
Here’s a LinkedIn comment about that issue from Craig Bryan. Dr. Bryan is a suicide researcher, professor at The Ohio State University, and author of “Rethinking Suicide.” In support of him and his research and thinking, I’d like to professionally say that although I lean away from reductionistic categorization of things, all signs point to the likelihood that Dr. Bryan has a very large brain.
The good news is that I feel validated by Dr. Bryan’s strong comments against categorizing suicide risk. But the bad news is that we all live in the real world and in the real world sometimes professionals have to do more than just swear about risk categorization—we have to actually make recommendations for or against hospitalization, consult with other professionals who want our opinion, and quoting me as saying that risk factor categorization is pure bullshit may not be the best and most professional option.
So . . . what are we to do? First, we parse Dr. Bryan’s comments. He’s not saying NEVER categorize risk or make risk estimates. He’s saying don’t categorize “negative screens as low risk” which is slightly different than don’t try to estimate risk. His message is that we have too many false negatives—where someone screens negative and then dies by suicide. In other words, we should not be confident and say negative screens are “low risk.” That’s different from throwing the baby out with the bathwater.
It might be easy to think that Dr. Bryan’s comments are discouraging. But I view him as just saying we should be careful professionals. To help with that, below is the excerpt on Suicide risk categorization and decision-making, from our textbook. If you’re in a situation where you have to make a professional recommendation about suicide risk, this information may be helpful. BTW, the reason I was inspired to post this excerpt is because the Korean participants were wonderful and asked lots of hard questions, including questions related to this topic.
Suicide Risk Categorization and Decision-Making
Throughout this chapter, we have acknowledged the limits of categorizing clients on the basis of risk. The current state of the science indicates that efforts to predict client suicides (i.e., categorize risk) are likely to fail. Nevertheless, when necessary—because of institutional requirements or client inability to collaborate on safety or treatment planning—all clinicians should be able to use their judgment to estimate risk and make disposition decisions for the welfare of the client. As a consequence, we review a suicide risk categorization and decision-making model next.
Consultation
Consultation with peers and supervisors serves a dual purpose. First, it provides professional support; dealing with suicidal clients is difficult and stressful; input from other professionals is helpful. For your health and sanity, you shouldn’t do work with suicidal clients in isolation.
Second, consultation provides feedback about appropriate practice standards. Should you need to defend your actions and choices following a suicide death, you’ll be able to show you were meeting professional standards. Consultation is one way to monitor, evaluate, and upgrade your professional competency.
Suicide Risk Assessment: An Overview
We reviewed an overwhelming number of suicide risk and protective factors earlier in this chapter. Generally, more risk factors equate to more risk. However, some risk factors are particularly salient. These include:
Previous attempts
A previous attempt is sometimes viewed as suicide rehearsal. Two previous attempts are especially predictive of suicide because they represent repeated intent. Also, when previous attempts were severe and the client was disappointed not to die, risk is high.
Command hallucinations
When clients are experiencing a psychotic state accompanied by command hallucinations (e.g., a voice that says, “You must die’), risk is at an emergency level.
Severe depression with extreme agitation
The combination of depression and agitation can be especially lethal. Agitation can take the form of extreme anxiety or extreme anger.
Protective factors
A single protective factor may outweigh many risk factors. But, it’s impossible to know the power of any individual protective factors without an in-depth discussion with your client. Engagement in therapy and collaboration on a safety plan (and the hope these behaviors signal) can substantially reduce risk.
Nature of Suicidal ideation
As discussed earlier, suicidal ideation is evaluated based on frequency, triggers, intensity, duration, and termination. Some clients live chronically with high suicidal ideation frequency, intensity, and duration—and are low risk. However, if ideation is frequent and intense and accompanied by intent and planning, risk is high.
Suicide Intent
Suicide intent is the factor most likely to move clients toward lethal attempts. Intent can be based on objective or subjective signs. Objective signs of intent include one (or more) previous lethal attempt(s). Subjective signs of intent can include a client rating of intent or client report of a highly lethal plan.
Clinical Presentation
How clients present themselves during sessions is revealing. Clients can be palpably hopeless, talk desperately about feelings of being trapped, and express painful and unremitting self-hatred or shame. But if clients have adapted to these experiences, they may not have accompanying intent and active planning. Observations of how clients talk about their psychological distress will contribute to your final decisions.
Final Decisions
Using a traditional assessment approach, you can estimate your client’s suicide risk as fitting into one of three categories:
Minimal to Mild: Client reports no suicidal thoughts or impulses. Client distress is minimal. Plan: Monitor client distress. If distress rises, or depressive symptoms emerge, re-assess for suicidality.
Moderate to High: Client reports suicidal ideation. As client distress, planning, risk factors, and intent increase, risk increases. Plan: Manage the situation with a collaborative safety plan. Depending on client preference, engaging family or friends as support may be advisable. Make sure firearms and lethal means are safely stored.
High to Extreme: Client reports suicidal ideation, plans, multiple risk factors (likely including a previous attempt), intent, and has access to lethal means. Engagement in treatment is minimal to non-existent. Plan: Treatment may include hospitalization and/or intensive outpatient therapy with a safety plan implemented in collaboration with family/friends. Make sure firearms and lethal means are safely stored.
************************
As always, please share your thoughts in the comments on this blog.
The place to click if you want to learn about psychotherapy, counseling, or whatever John SF is thinking about.