My apologies for the late notice, but I’m doing a free, online, one-hour talk tomorrow, 3/4/2026 at 2-3pm Mountain time. Sponsored by the Center for Children, Families, and Workforce Development and MAPP-Net, the talk is titled, “Ten things Everyone Should Know about Suicide, Mental Health, and Happiness.” Here’s the link:
Warning: this is not my most uplifting talk. the first half focuses mostly on the “Wicked Problem” of suicide. The good news is that I do end on Happiness!
Whether you attend or not (it’s free!), thanks for being someone who’s working to make the world a better, kinder, and more eudaimonically happy place.
You may be wondering (I know I am), what does a glimpse and quote from the illustrious Laura Perls have to do with suicide prevention slides for North Carolina State University?
If you have thoughts on the connection, please share. I see a connection, but maybe it’s just because I wanted to post both these things. First, here’s a bit of content from Laura Perls from our Counseling and Psychotherapy Theories text.
***************************************
Although the contributions of Laura Posner Perls to Gestalt therapy practice were immense, she never receives much credit, partly due to the flamboyant extraversion of Fritz and partly because her name, somewhat mysteriously (at least to us), is not on many publications. She does, however, comment freely on Fritz’s productivity at the twenty-fifth anniversary of the New York Institute for Gestalt Therapy (an organization that she co-founded with Fritz).
Without the constant support from his friends, and from me, without the constant encouragement and collaboration, Fritz would never have written a line, nor founded anything. (L. Perls, 1990, p. 18)
REFLECTIONS
We hear resentment in the preceding quotation from Laura Perls. We feel it too, because we’d like to know more about Laura and for her to have gotten the credit she deserved. If you want more Laura, here’s a nice tribute webpage: https://gestalt.org/laura.htm?ya_src=serp300. And here’s a quotation from her (obtained from the webpage and compiled by Anne Leibig): “Real creativeness, in my experience, is inextricably linked with the awareness of mortality. The sharper this awareness, the greater the urge to bring forth something new, to participate in the infinitely continuing creativeness in nature. This is what makes out of sex, love; out of the herd, society; out of wheat and fruit, bread and wine; and out of sound, music. This is what makes life livable and incidentally makes therapy possible.”
Now, don’t you want to hear more from Laura?
*******************************************
And here’s the North Carolina State University link:
Now that I’m immersed in positivity every day as the Director of the Center for the Advancement of Positive Education, I think I’ve become weirder.
Some of you, including my sisters and brothers-in-law may be wondering, “Wait. How could John become any MORE weird than he already is?”
You know what they say: “All things are possible!” [Actually, I don’t know why I just wrote all things are possible, because, even in my most positive mental states, I don’t believe that BS. All things are not possible. I could make a list of impossible things, but I’ve already digressed.]
Here’s what I mean by me becoming even weirder.
I find myself more easily hearing and seeing the pervasive negative narratives emerging around us. I could make another long list of all the bad ideas (negative narratives) I’m noticing (think: “fight or flight”), but I’ll limit myself to one example: The “Trigger warning.”
Trigger warnings are statements that alert listeners or viewers (or people attending my suicide assessment workshops) to upcoming intense and potentially emotionally activating content. Over the past 10ish years, we’ve all started giving and receiving trigger warnings from time to time, now and then. A specific example, “The next segment of this broadcast includes gunfire” or “In my lecture I will be talking about mental health and suicide.”
As a college professor in a mental health-related discipline, I became well-versed in providing trigger warnings. . . and have offered them freely. Because some people have strong and negative emotional reactions to specific content, providing trigger warnings has always made good sense. The point is to alert people to intense content so they can take better care of themselves or opt out (stop listening/viewing). Trigger warnings are important and, no doubt, useful for helping some people prepare for emotionally activating content.
As a college professor, I’m also obligated to keep up with the latest research. Unfortunately, the research on trigger warnings isn’t very supportive of trigger warnings. Argh! In general, it appears that trigger warnings sensitize people and might make some people more likely to have a negative emotional response. You can read a 2024 meta-analysis on trigger warning research here: https://journals.sagepub.com/doi/10.1177/21677026231186625
In response to the potential adverse effects of trigger warnings, I came up with a clever idea: I started giving trigger warnings for my trigger warnings. These were something like, “Because research suggests that trigger warnings can make you more reactive to negative content, I want to give you a trigger warning for my trigger warning and encourage you to not let my warning make you more sensitive than you already would be.”
Then, about a year ago, I had an epiphany. [I feel compelled to warn you that my epiphany might just be common sense, but it felt epiphany-like to me]
I realized—perhaps aided by my experiences training to do hypnosis—that trigger warnings might be functioning as negative suggestions, implying that people might not be able to handle the content and priming them to notice and focus on their negative reactions.
Given my epiphany, I was energized—as the solution-focused people like to say—to do something different. The different thing I settled on was to invent “The Strength Warning.”
[Here’s where I digress again to pitch a podcast. Paula Fontenelle, an all-around wonderful, kind, and competent professional, has a new podcast called, Relating to AI. And, lucky me, I got to be one of her very first guests. And, lucky Paula (joking now), she got to have me start her podcast interview by explaining and demonstrating the strength warning. Consequently, if you’re interested in AI and/or in hearing me demonstrate the strength warning, the link to Paula’s podcast is here: https://www.youtube.com/watch?v=MHDIYrXw_2Y]
Although watching/listening to me give the strength warning with Paula is way more fun, I will also describe it below.
For strengths warnings, I say things like this.
In addition to warning you about sensitive content coming up, I also want to give you a Strength Warning. A strength warning is mostly the opposite of a trigger warning. I want you to watch out for the possibility that being here together in this lecture and with your colleagues might just make you notice yourself feeling stronger, feeling better, feeling more prepared, feeling more knowledgeable, and maybe even feeling smarter. So . . . watch for that, because I think you might even be stronger than you think you are.
Please, let me know what you think about my invention of the strength warning. I encourage you to try it out when you’re teaching or presenting.
I also encourage you to try out Paula’s new podcast. If you do, you might feel smarter, stronger, and more prepared to face the complicated issue of having AI intrude on our lives.
Today, Tammy Tolleson Knee and completed day 1 of a 2-day course on Strengths-Based Suicide Assessment and Interventions in Schools at the Buffalo Hide Academy of Browning Public Schools on the Blackfeet Reservation. We are beyond happy for this opportunity. It’s the first time for Tammy and I to present together (for two days!). As frosting on the presentation cake, Rita is here with us, watching, listening, heckling, and guiding.
In case you haven’t heard, Browning Public Schools and their staff have already started integrating strengths-based suicide prevention work into their programming. Two of our former University of Montana school counseling graduates, Sienna and Charlie Speicher are at the center of this work. Sienna and Charlie have already taught strengths-based courses through Blackfeet Community College, and they founded the Firekeeper Alliance. Here’s the Firekeeper Alliance Mission Statement:
Our mission is to cultivate resources, attention, and awareness to ultimately transform perspectives regarding suicidal distress in Indian Country and to help reduce suicide rates in our communities. We believe that mainstream and current approaches of suicide assessment and intervention struggle to meet the unique needs of Tribal populations. The Firekeeper Alliance promotes a different set of strengths-based, decolonized ideals around suicidal behavior. We believe that systemic and cultural shifts in the clinical community are necessary to truly make a positive change.
The Firekeeper Alliance also focuses on several areas, including offering strengths-based approaches to counseling, as in the following:
Offer individual and group counseling sessions utilizing evidence-based therapies which are effective in addressing suicidality.
Promote assessment techniques and interventions that elicit protective factors and a resilient spirit.
Administer assessment instruments that screen for strengths, character assets, and benevolent experience to depathologize suicidal distress.
Advocate for strengths based assessment and intervention approaches to be used in conjunction with cultural healing mechanisms.
Back to our training. . .here are the ppts that Tammy and I developed. There are SO MANY, but then again, we’re covering two whole days!
In closing, I want to give a big shout-out to Browning Public Schools (BPS) for collaborating with us (the Center for the Advancement of Positive Education; aka CAPE) to bring this training to Browning. Not only do we have a dozen or so school counselors in the room, we’ve also got a dozen or so administrative staff, including principals and the BPS superintendent. We had a blast today and are looking forward to more meaningful fun tomorrow!
Yesterday I was in Arkansas with the Arkansas Psychological Association talking about Strengths-based Suicide Assessment. And today I’m in Philly, along with Dr. Umit Arslan (and missing Tammy Tolleson-Knee) talking about it again–at the Association of Counselor Education and Supervision conference.
Unfortunately, Tammy’s efforts to get here were foiled by a particular airline fiasco, but we’re carrying on! We miss you Tammy!
This is a fact-focused post. I’d like to be verbally clever, but I’d like even more to get you all this information on what’s happening at the Phyllis J. Washington Center for the Advancement of Positive Education.
We’re building our staff, our website, and plans for this fall. You may want some or all of the following on your calendar. . .or to share them with people whom you think would be interested.
A New University of Montana Course
Kim Parrow and Tammy Tolleson-Knee developed a syllabus for a EDU 291 course called, The Psychology of Happiness. This is a late-start, face-to-face course that begins the week of September 15. If you’re a UM student or know one who might want to experience a positive psych course, here’s the flyer:
Dylan Wright and Kim Parrow will be taking the lead on the fall semester Happiness for Educators (HFE) course. Data attesting to the value of this course continue to pour in. With 150+ enrolled this summer, we’ve now had well over 400 Montana educators complete the course. A big thanks to the Arthur M. Blank Family Foundation for supporting Montana educators. And Go Falcons! Here’s a flyer for the HFE course:
Dylan and Tammy are also working with local schools to infuse principles of positive education as methods to improve educator well-being. They’re starting with the Potomac School District. . . and have named their approach, “The Potomac Model.” Thanks to Emily Sallee, the shiny new Potomac superintendent for collaborating with us. If your school district would like to collaborate with us, Dylan Wright is your best contact: dylan.wright@mso.umt.edu
As for myself, I’ve got a few gigs coming up as well. Below are the ones I’m thinking about today!
September 16 – Youth Summit Keynote in Kalispell – 9:15-10am – Flathead Valley Community College – Thanks to the Nate Chute Foundation for organizing this.
The Bad News Brain: Why It Feels So Hard and What You Can Do
Maintaining positive mental health is naturally difficult—for nearly everyone. The good news is that if you struggle with mental health, you’re not alone. The bad news is that your brain often likes to focus on bad news, bad moods, and bad social interactions. The other good news is that after this presentation, you will know several ways your brain tries to trick you into feeling worse. You will also know several strategies for dealing with your pesky bad-news-brain.
September 25 – Presentation at the State CASA Conference in Butte – 11am-12:30pm – Finlen Hotel. Thanks to the Montana State CASA people for their support of Montana children.
Ten Things Everyone Should Know About Children’s Mental Health and Happiness
After 40+ years as a mental health professional, John Sommers-Flanagan has discovered an array of myths that inadvertently contribute to ever-rising mental health problems in children and teenagers. In this presentation for Montana CASA, we will go on a rollercoaster ride through three principles of positive psychology and 10 (or maybe 11) misconceptions about mental health and happiness that will knock your socks off (not literally). And perhaps, as we engage in the learning process together, you may be inspired to think a little differently about how to grow positive mental health and happiness in youth.
September 27 – Presentation on Happiness in Absarokee, MT – 2-5pm – Cobblestone School. Thanks to the Cobblestone Preservation Committee for sponsoring this event.
Tools for Living Your Best Life: A Happiness Primer
October 9 – Grand Rounds presentation on Strengths-Based Suicide, the University of Arkansas for Medical Sciences (UAMS) in Little Rock, AR – 4pm
October 10 – Full-day workshop on Strengths-Based Suicide for the Arkansas Psychological Association in Little Rock, AR – 8:30am-4pm – Holiday Inn Presidential. Thanks to Dr. Margaret Rutherford, President of the Arkansas Psychological Association for making these presentations happen.
Integrating Strengths-Based and Traditional (Medical Model) Approaches to Suicide Assessment and Treatment
Traditional suicide assessment tends to be a top-down information-gathering process wherein healthcare or prevention professionals use questionnaires and clinical interviews to determine patient or client suicide risk. This approach may not be the best fit for clients who are suicidal, who have experienced historical trauma, or are experiencing current oppression or marginalization. In this presentation, John Sommers-Flanagan will review principles of a strengths-based approach to suicide prevention, assessment, and treatment. He will also discuss how to be more sensitive, empowering, collaborative, and how to leverage individual and cultural strengths when working with people who are potentially suicidal. You will learn at least five practical strengths-based strategies for initiating conversations about suicide, conducting culturally-sensitive assessments, and implementing suicide interventions.
October 11 — Round Table presentation with Tammy Tolleson-Knee and Umit Arslan at the Association for Counselor Education and Supervision conference in Philly.
Shifting from Risk-Focused to Resilience-Oriented Approaches in Youth Mental Health Assessments
Traditional suicide assessments often focus on pathology and risk, overlooking client strengths and resilience. Effective prevention goes beyond simply identifying suicidal thoughts—it involves fostering awareness, developing coping skills, and strengthening a person’s belief in their ability to navigate challenges. This session examines strengths-based suicide assessment from three perspectives: (1) distinguishing scientific research from myths and implementing evidence-based steps, (2) recognizing countertransference as a barrier to strengths-based suicide intervention and developing effective coping strategies, and (3) evaluating how strengths-based approaches can promote a holistic, resilience-oriented approach to youth mental health. Participants will engage in discussions, case vignettes, and interactive learning activities, gaining practical applications for counselor education and supervision.
October 29 – Keynote for Montana Healthcare Foundation in Bozeman – 10:05-10:55am – Strand Union Building, Montana State University. Thanks to the fabulous staff of the Montana Healthcare Foundation for organizing this amazing event.
The Bad News Brain: Why We Must Force Ourselves to Embrace Well-Being and Positivity
The human brain is naturally interested in bad news. Several deep psychological truths make this so. In this keynote speech, we will focus on what makes it so hard to maintain a positive focus. Then, we will force ourselves to orient toward the positive—even if only briefly—to explore practical ways we can grow well-being in Montana together.
October 29 – Breakout Workshop for Montana Healthcare Foundation in Bozeman – 2-3:50pm – Strand Union Building, Montana State University.
Evidence-Based Strategies for Integrating Strengths-Based Approaches into Mental Health Care
Beginning with a cognitive-behavioral model of mood management, this breakout workshop will focus on evidence-based strategies that can complement traditional medical model approaches to mental health care. Evidence-based strategies will include: (a) witnessing inspiration, (b) therapeutic writing, (c) savoring, and more. Discussion and reflection will include how to collaboratively leverage individual, family, community, and cultural strengths when providing mental health support.
November 12-13 – 1 credit college course for Blackfeet Community College in Browning, MT – 8am-4:30pm (two days) at BCC. Thanks to Charlie Speicher WBH school counselor and founder of the Firekeeper Alliance for creating this opportunity.
Strengths-Based Suicide Assessment and Interventions in Schools
Traditional suicide assessments tend to be top-down information-gathering procedures wherein healthcare, school, or prevention professionals use questionnaires and clinical interviews to determine suicide risk. This approach may not be the best fit for schools, students, youth who are suicidal, or people who have experienced historical trauma, or are experiencing current oppression or marginalization. In this course, John Sommers-Flanagan and Tamara Tolleson-Knee will review principles of a strengths-based approach to suicide prevention, assessment, and interventions. They will share background research and historical practice, including the growing rationale for using strengths-based approaches with people who are feeling vulnerable. This course will include counseling and assessment demonstrations, video clips, and opportunities for participants to practice specific strengths-based suicide assessment and intervention strategies. In particular, there will be discussions about how to leverage individual, family, community, and cultural strengths when working with students who may be suicidal. Participants will learn numerous strengths-based strategies for initiating conversations about suicide, conducting strengths-based assessments, and implementing suicide interventions.
December 5 – Zoom Lecture for North Carolina State University – 5:30-7pm EST. Thanks to Dr. Angel Dowden for organizing this presentation.
Effective Approaches to Suicide Intervention and Prevention in Schools
Traditional suicide assessments tend to be top-down information-gathering procedures wherein healthcare, school, or prevention professionals use questionnaires and clinical interviews to determine suicide risk. This approach may not be the best fit for schools, students, youth who are suicidal, or people who have experienced historical trauma, or are experiencing current oppression or marginalization. In this Zoom workshop, John Sommers-Flanagan will review principles of a strengths-based approach to suicide prevention, assessment, and interventions. This workshop will include at least one assessment demonstration, a video clip, and brief opportunities for participants to practice specific strengths-based suicide assessment and intervention strategies. The overall focus is on how to leverage individual, family, community, and cultural strengths when working with students who may be suicidal.
If you’ve read this far, I am completely gob-smacked. Have a fabulous day!
Last Friday night (or Saturday morning in South Korea), I had the honor and privilege of spending three hours online with 45 South Korean therapists. We were talking, of course, about strengths-based suicide assessment and treatment. Given my limited Korean language skills (is it accurate to say my language skills are limited if I can’t say or comprehend ANYTHING in Korean?), I had a translator. Although I couldn’t tell anything about the translation accuracy, my distinct impression was that she was absolutely amazing.
I had a friend ask how I happened to get invited to present to Korean therapists. My main response is that I believe the time is right (aka Zeitgeist) for greater integration of the strengths-based approach into traditional suicide assessment and treatment. The person who recruited me was Dr. Julia Park, another absolutely amazing, kind, and competent South Korean person, who also happens to hold an Adlerian theoretical orientation. Thanks Julia!
Just for fun, I wish I had my Korean translated ppts to share here. They’re unavailable, and so instead I’m sharing an excerpt from Chapter 10 (Suicide Assessment Interviewing) of our Clinical Interviewing (2024) textbook. The section I’m featuring is the part where we review issues and procedures around suicide risk categorization and decision-making.
You may already know that some of the latest thinking on suicide risk assessment is that we should not use instruments like the Columbia to categorize risk. You also may know that not only am I a believer in this latest thinking, I can be wildly critical of efforts to categorize suicide risk. . . so much so that I often end up using profanity in my professional presentations. Of course, because the context is a professional presentation, I only use the highly professional versions of profanity.
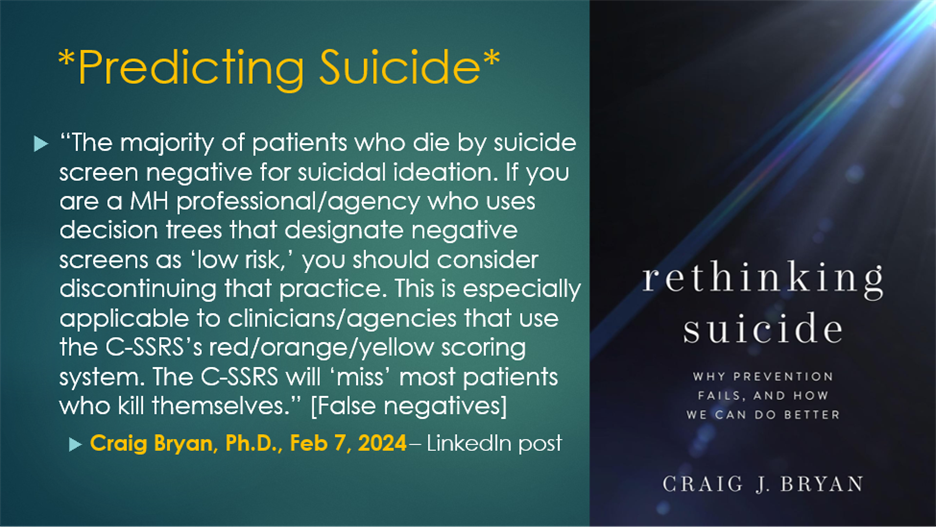
Here’s a LinkedIn comment about that issue from Craig Bryan. Dr. Bryan is a suicide researcher, professor at The Ohio State University, and author of “Rethinking Suicide.” In support of him and his research and thinking, I’d like to professionally say that although I lean away from reductionistic categorization of things, all signs point to the likelihood that Dr. Bryan has a very large brain.
The good news is that I feel validated by Dr. Bryan’s strong comments against categorizing suicide risk. But the bad news is that we all live in the real world and in the real world sometimes professionals have to do more than just swear about risk categorization—we have to actually make recommendations for or against hospitalization, consult with other professionals who want our opinion, and quoting me as saying that risk factor categorization is pure bullshit may not be the best and most professional option.
So . . . what are we to do? First, we parse Dr. Bryan’s comments. He’s not saying NEVER categorize risk or make risk estimates. He’s saying don’t categorize “negative screens as low risk” which is slightly different than don’t try to estimate risk. His message is that we have too many false negatives—where someone screens negative and then dies by suicide. In other words, we should not be confident and say negative screens are “low risk.” That’s different from throwing the baby out with the bathwater.
It might be easy to think that Dr. Bryan’s comments are discouraging. But I view him as just saying we should be careful professionals. To help with that, below is the excerpt on Suicide risk categorization and decision-making, from our textbook. If you’re in a situation where you have to make a professional recommendation about suicide risk, this information may be helpful. BTW, the reason I was inspired to post this excerpt is because the Korean participants were wonderful and asked lots of hard questions, including questions related to this topic.
Suicide Risk Categorization and Decision-Making
Throughout this chapter, we have acknowledged the limits of categorizing clients on the basis of risk. The current state of the science indicates that efforts to predict client suicides (i.e., categorize risk) are likely to fail. Nevertheless, when necessary—because of institutional requirements or client inability to collaborate on safety or treatment planning—all clinicians should be able to use their judgment to estimate risk and make disposition decisions for the welfare of the client. As a consequence, we review a suicide risk categorization and decision-making model next.
Consultation
Consultation with peers and supervisors serves a dual purpose. First, it provides professional support; dealing with suicidal clients is difficult and stressful; input from other professionals is helpful. For your health and sanity, you shouldn’t do work with suicidal clients in isolation.
Second, consultation provides feedback about appropriate practice standards. Should you need to defend your actions and choices following a suicide death, you’ll be able to show you were meeting professional standards. Consultation is one way to monitor, evaluate, and upgrade your professional competency.
Suicide Risk Assessment: An Overview
We reviewed an overwhelming number of suicide risk and protective factors earlier in this chapter. Generally, more risk factors equate to more risk. However, some risk factors are particularly salient. These include:
Previous attempts
A previous attempt is sometimes viewed as suicide rehearsal. Two previous attempts are especially predictive of suicide because they represent repeated intent. Also, when previous attempts were severe and the client was disappointed not to die, risk is high.
Command hallucinations
When clients are experiencing a psychotic state accompanied by command hallucinations (e.g., a voice that says, “You must die’), risk is at an emergency level.
Severe depression with extreme agitation
The combination of depression and agitation can be especially lethal. Agitation can take the form of extreme anxiety or extreme anger.
Protective factors
A single protective factor may outweigh many risk factors. But, it’s impossible to know the power of any individual protective factors without an in-depth discussion with your client. Engagement in therapy and collaboration on a safety plan (and the hope these behaviors signal) can substantially reduce risk.
Nature of Suicidal ideation
As discussed earlier, suicidal ideation is evaluated based on frequency, triggers, intensity, duration, and termination. Some clients live chronically with high suicidal ideation frequency, intensity, and duration—and are low risk. However, if ideation is frequent and intense and accompanied by intent and planning, risk is high.
Suicide Intent
Suicide intent is the factor most likely to move clients toward lethal attempts. Intent can be based on objective or subjective signs. Objective signs of intent include one (or more) previous lethal attempt(s). Subjective signs of intent can include a client rating of intent or client report of a highly lethal plan.
Clinical Presentation
How clients present themselves during sessions is revealing. Clients can be palpably hopeless, talk desperately about feelings of being trapped, and express painful and unremitting self-hatred or shame. But if clients have adapted to these experiences, they may not have accompanying intent and active planning. Observations of how clients talk about their psychological distress will contribute to your final decisions.
Final Decisions
Using a traditional assessment approach, you can estimate your client’s suicide risk as fitting into one of three categories:
Minimal to Mild: Client reports no suicidal thoughts or impulses. Client distress is minimal. Plan: Monitor client distress. If distress rises, or depressive symptoms emerge, re-assess for suicidality.
Moderate to High: Client reports suicidal ideation. As client distress, planning, risk factors, and intent increase, risk increases. Plan: Manage the situation with a collaborative safety plan. Depending on client preference, engaging family or friends as support may be advisable. Make sure firearms and lethal means are safely stored.
High to Extreme: Client reports suicidal ideation, plans, multiple risk factors (likely including a previous attempt), intent, and has access to lethal means. Engagement in treatment is minimal to non-existent. Plan: Treatment may include hospitalization and/or intensive outpatient therapy with a safety plan implemented in collaboration with family/friends. Make sure firearms and lethal means are safely stored.
************************
As always, please share your thoughts in the comments on this blog.
Last week was a blur. On Wednesday, I did a break-out session for the Montana Prevent Child Abuse and Neglect conference in Helena. I’ve been to this conference multiple times and always deeply appreciate the amazing people in Montana and beyond who are dedicated to the mission of preventing child abuse and neglect. For the break-out, I presented on “Ten Things Everyone Should Know About Mental Health, Suicide, and Happiness.” This is one of my favorite newish topics and I felt very engaged with the 120+ participants. A big thanks to them.
Before the session, I felt a bit physically “off.” Overnight, the “off” symptoms developed into a sore throat and cough. This would NOT have been a problem, except I was scheduled for the hour-long closing conference keynote on Thursday. The good news is that I had zero fever and it was NOT Covid. The bad news was my voice was NOT good. I did the talk “In Pursuit of Eudaimonia” with 340ish attendees and got through it, but only with the assistance of a hot mic.
I had to cancel my Friday in Missoula and ended up in Urgent Care, with a diagnosis of bronchitis or possibly pneumonia, which was rather unpleasant over the weekend.
Having recovered (mostly), by yesterday, I recorded a podcast (Justin Angle’s “A New Angle” on Montana Public Radio) at the University of Montana College of Business. Thanks to a helpful pharmaceutical consult with a helpful woman at Albertsons, I had just the right amount of expectorant, later combined with a strong cough suppressant, to make it through 90 minutes of fun conversation with Justin without coughing into the podcast microphone. We talked about “Good Faith” in politics, society, and relationships. The episode will air in early June.
And now . . . I’m in beautiful Butte, Montana, where I’m doing an all-day (Thursday) workshop for the Montana Sex Offender Treatment Association. . . on Strengths-Based Suicide Assessment and Treatment . . . at the Copper King Hotel and Convention Center. Not surprisingly, having slept a bit extra the past five days, I’m up and wide awake at 4:30am, with not much to do other than post a pdf of my ppts for the day. Here they are:
Thanks for reading and thanks for being the sort of people who are, no doubt, doing what you can to make Montana and the world a little kinder and more compassionate place to exist.
Be well.
The place to click if you want to learn about psychotherapy, counseling, or whatever John SF is thinking about.