Tammy, Dylan, and I are on our way to Polson, MT this morning to provide a 6-hour workshop on Counseling Youth.
The workshop title, “Tough Kids, Cool Counseling,” is a remnant of days gone by. Back in 1996, as Rita and I were driving from Missoula to Absarokee, we came up with that title, which we published as a book in 1997. The second edition came out in 2007.
For many years, we argued about who came up with what we considered a very nice title. I thought it was my idea. Rita thought it was hers. We were both equally shocked at each others’ claims. Have you ever had that experience with a romantic partner?
But, a few years after publishing the second edition, I gave up all claims to the title, because I suddenly realized that the title was neither nice nor cool. Constructing youth problems as “in them” was not good and not right. The title labeled the youth as “tough,” in essence, blaming them for their problems.
For the past two decades, I’ve seen youth problems differently. Now, I avoid using the phrase “Tough kids.” Instead, I advocate for framing the issues as “kids in tough life and personal situations.” I’ve decided that going to counseling is just another tough situation that many youth are forced into.
So why am I still using this title? I use it because I like to make the point–after using the phrase Tough Kids for the first five minutes–that I’ve stopped using it and that I won’t use it for the rest of the presentation and that we should all give it up together, and not even THINK about tough kids.
With that fun anecdote out of the way, I’m looking forward to a fun day of mutual learning with therapists who work for the Confederated Salish & Kootenai Tribes. And. . .here’s a pdf of the very long powerpoint slide deck.
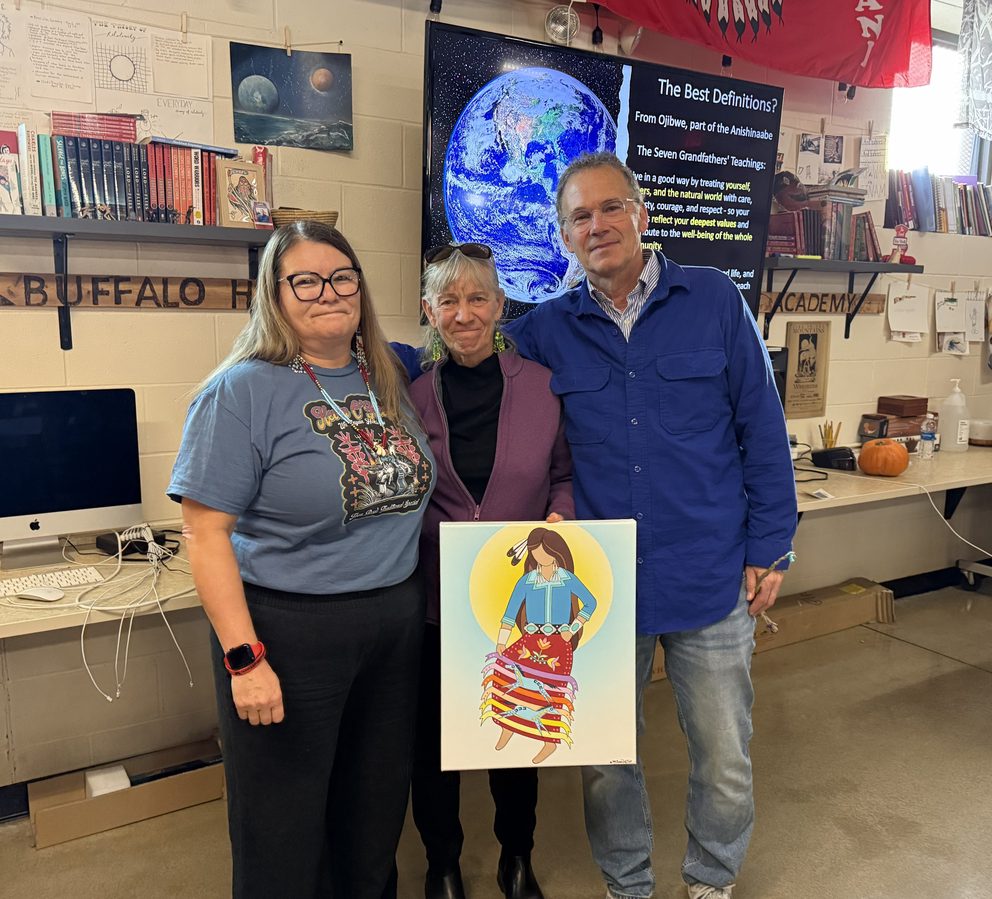
This photo is of Lynnel Bullshoe gifting Rita beautiful Indigenous art at a two-day workshop in Browning on the Blackfeet Reservation.
With all the politicizing and media activity around DEI, I think it’s easy to get confused and polarized on DEI issues. Last October, when talking with a friend at a conference in Philly, my friend told a story that I found wonderfully clarifying about DEI. In my previous Theories Preface post, I didn’t include her anecdote–which is one of my favorites–because I didn’t have permission then. But I have permission now, so here’s the missing anecdote:
Recently, a friend of ours told us a story about being asked to deliver a keynote speech for a state school counselor association event. A board member recommended that she “go light on DEI.” Perhaps our friend interpreted that as “You’ve got the green light on DEI,” as the beginning of her speech went something like this:
I was asked to go light on DEI, so I’d like to start by saying, I recently heard someone say that the opposite of diversity is uniformity. The opposite of equity is inequity. The opposite of inclusion is exclusion. And the opposite of anti-racism is racism. I sincerely hope it’s safe to say that as school counselors, none of us want uniformity, inequities, or exclusionary and racist practices.
She went on to remind the audience that we cannot take DEI out of our work, that it is our professional and ethical duty to continuously examine our biases, assumptions, and beliefs, and engage in the ongoing work of self-reflection, learning, and unlearning (J. V. Taylor, personal communication, October 11, 2025).
I love this clear, concise, and beautiful analysis of what is NOT DEI.
Some weeks are like that. I’d share the details, but that would spoil the surprise. Besides, I’m really not into giving hate email (or hate mail or hate social media posts) any oxygen.
But today I got an email alert from “A New Angle” the radio-podcast show hosted by Dr. Justin Angle, a professor in the College of Business Administration at the University of Montana. The email was alerting me to the imminent airing of Part 2 of my discussion of “Good Faith” with Just on his renowned radio show. I was grateful for the alert; it also reminded me of my hate email, because the hate email came from someone who listened to Part 1 of our Good Faith conversation and consequently felt that special sort of inspiration that moves people to write hate emails.
I’ve known Justin from a distance for a while. We’re both at the University of Montana, so, you know, there’s been a little chat here, a little chat there. I’ve also known of him growing his small podcast into a big deal on Montana Public Radio and Yellowstone Public Radio. Justin’s show is excellent.
What I didn’t know is the depth and breadth of Justin’s intelligence. I also didn’t know that he’s a fabulous interviewer. I discovered his amazing intelligence and fabulousness when I sat down with him this past May to record a show with him on Good Faith. We talked comfortably for what felt like a long time. Not only did it feel like a long time, it was a long time! It was so long that Justin turned our conversation into a two-part episode for his radio show.
Here’s the email I received:
This week is part two of our conversation with John Sommers-Flanagan, director of the Center for the Advancement of Positive Education at the University of Montana’s Phyllis J. Washington College of Education.
John and Justin pick up where they left off last week talking about how lying and parenting intersect, the concept of confirmation bias and the risks of AI-generated content and building relationships with AI.
Here’s a link to Part 2 of our conversation. It’s also live at 7:30pm tonight (Thursday, June 19, 2025) on Montana Public Radio:
I’ve spent the better part of the past two weeks doing presentations in various locations and venues. I did five presentations in Nebraska, and found myself surprisingly fond of Lincoln and Kearney Nebraska. On Thursday I was at a Wellness “Reason to Live” conference with CSKT Tribal Services at Kwataqnuk in Polson. Just now I finished an online talk with the Tex-Chip program. One common topic among these talks was the title of this blog post. I have found myself interestingly passionate about the content of this particular. . . so much so that I actually feel energized–rather than depleted–after talking for two hours.
Not surprisingly, I’ve had amazingly positive experiences throughout these talks. All the participants have been engaged, interesting, and working hard to be the best people they can be. Beginning with the Mourning Hope’s annual breakfast fundraiser, extending into my time with Union Bank employees, and then being with the wonderful indigenous people in Polson, and finally the past two hours Zooming with counseling students in Texas . . . I have felt hope and inspiration for the good things people are doing despite the challenges they face in the current socio-political environment.
If you were at one of these talks (or are reading this post), thanks for being you, and thanks for contributing your unique gifts to the world.
For your viewing pleasure, the ppts for this talk are linked here.
Tomorrow morning, three counseling interns and I will hit the road for Ronan, where we’ll spend the day with the staff of CSKT Tribal Health. We are honored and humbled to engage in a conversation about how to make the usual medical model approach to suicide be more culturally sensitive and explicitly collaborative.
Why Do We Need a Strengths-Based Approach to Suicide Assessment and Treatment?
Imagine this: You’re living in a world that seems like it would just as soon forget you exist. Maybe your skin color is different than the dominant people who hold power. Maybe you have a disability. Whatever the case, the message you hear from the culture is that you’re not important and not worthy. You feel oppressed, marginalized, unsupported, and as if much of society would just as soon have you become invisible or go away.
In response, you intermittently feel depressed and suicidal. Then, when you enter the office of a health or mental health professional, the professional asks you about depression and suicide. Even if the professional is well-intended, judgment leaks through. If you admit to feeling depressed and having suicidal thoughts, you’ll get a diagnosis that implies you’re to blame for having depressing and suicidal thoughts.
The medical model overfocuses on trying to determine: “Are you suicidal?” The medical model is also based on the assumption that the presence of suicidality indicates there’s something seriously wrong with you. But if we’re working with someone who has been or is currently being marginalized, a rational response from the patient might be:
“As it turns out, I’ve internalized systemic and intergenerational racism, sexism, ableism, and other dehumanizing messages from society. I’ve been devalued for so long and so often that now, I’ve internalized societal messages: I devalue myself and wonder if life is worth living. And now, you’re blaming me with a label that implies I’m the problem!”
No wonder most people who are feeling suicidal don’t bother telling their health professionals.
When I think of this preceding scenario, I want to add profanity into my response, so I can adequately convey that it’s completely unjust to BLAME patients for absorbing repeated negative messages about people who look like or sound like or act like them. WTH else do you think should happen?
This is why we need to integrate strengths-based principles into traditional suicide assessment and prevention models. Of course, we shouldn’t use strengths-based ideas in ways that are toxically positive. We ALWAYS need to start by coming alongside and feeling with our patients and clients. As it turns out, if we do a good job of coming alongside patients/clients who are in emotional pain, natural opportunities for focus on strengths and resources, including cultural, racial, sexual, and other identities that give the person meaning.
I’m reminded of an interview I did with an Alaskan Native person from the Yupik tribe. She talked at length about her depression, about feeling like a zombie, and past and current suicidal thoughts. Eventually, I inquired: “What’s happening when you’re not having thoughts about suicide?” She seemed surprised. Then she said, “I’d be singing or writing poetry.” I instantly had a sense that expressing herself held meaning for her. In particular, her singing Native songs and contemporary pop songs became important in our collaborative efforts to build her a safety plan.
This coming Wednesday morning I have the honor of presenting as the keynote speaker for the Maryland Department of Health 36th Annual Suicide Prevention Conference. During this keynote, I’ll share more ideas about why a strengths-based model is a good fit when working with diverse clients who are experiencing suicidal thoughts and impulses.
With all that said, here’s the title and abstract of my upcoming presentation.
Strengths-Based Assessment, Treatment, and Prevention with Diverse Populations
Traditional suicide assessment tends to be a top-down information-gathering process wherein healthcare or prevention professionals use questionnaires and clinical interviews to determine patient or client suicide risk. This approach may not be the best fit for people from populations with historical trauma, or for people who continue to experience oppression or marginalization. In this presentation, John Sommers-Flanagan will review principles of a strengths-based approach to suicide prevention, assessment, and treatment. He will also discuss how to be more sensitive, empowering, collaborative, and how to leverage cultural strengths when working with people who are potentially suicidal. You will learn at least three practical strengths-based strategies for initiating conversations about suicide, conducting culturally-sensitive assessments, and implementing suicide interventions—that you can immediately use in your prevention work.
The place to click if you want to learn about psychotherapy, counseling, or whatever John SF is thinking about.