This past week I had the honor and privilege of offering four presentations, one each on Monday, Tuesday, Wednesday, and Thursday.
Monday was a Zoom date with a counseling class at West Virginia University.
Tuesday was an exciting in-person presentation for the University of Montana MOLLI program, kicking off our small group experiential Evidence-Based Happiness course for older adults. It was phenomenal. The older adults always bring it. One–among many–highlights was an 88 -year-old guy who, in the midst of the Three-Step Emotional Change Trick, shared about how he “Honored” his emotions by joining a grief group after his wife died (3 years ago). His sharing was beautiful and perfect.
Wednesday was my annual visit to Dr. Timothy Nichols’s Honors College course on LOVE. Dr. Nichols happens to be the Dean of the Honors College and one of the coolest and kindest and most enthused people on the planet. Mostly I go every year just to hear him introduce me. In truth, I also go because the topic and the students are INCREDIBLE. I think it may have been the best LOVE lecture EVER. I’d post the ppts here, but my computer crashed yesterday, and the U of M IT people (who are always very nice) are now attempting “data recovery.” Argh!
Thursday I got to hang out for two hours with the Graduate Students of the University of Montana Psychology Club. This was yet another fun experience with a group of students who are all simply brilliant. To top it off, a couple of my favorite people (and Psych faculty), Bryan Cochran and Greg Machek also attended. . . providing the precise level of sarcasm and humor that made the experience practically perfect. Here are the Psych Club’s ppts, which I happened to have on a flash drive:
I’ve been in repeated conversations with numerous concerned people about the risks and benefits of suicide screenings for youth in schools. Several years ago, I was in a one-on-one coffee shop discussion of suicide prevention with a local suicide prevention coordinator. She said, more as a statement than a question, “Who could be against school-based depression and suicide screenings?”
I slowly raised my hand, forced a smile, and confessed my position.
The question of how and why I’m not in favor of school-based mental health and suicide screenings is a complex one. On occasion, screenings will work, students at high-risk will be identified, and tragedy is averted. That’s obviously a great outcome. But I believe the mental health casualties from broad, school-based screenings tend to outweigh the benefits. Here’s why.
Early identification of depression and suicide in youth will result in early labeling in school systems; even worse, young people will begin labeling themselves as being “ill” or “defective.” Those labels are sticky and won’t support positive outcomes.
Most youth who experience depressive symptoms and suicide ideation are NOT likely to die by suicide. Odds are that students who don’t report suicidal ideation are just as likely to die by suicide. As the scientists put it, suicidal ideation is not a good predictor of suicide. Also, depression symptoms generally come and go among teenagers. Most teens will recover from depressive symptoms without intensive interventions.
After a year or two of school-based screenings, the students will know the drill. They will realize that if they endorse depression symptoms and suicidal items that they’ll have to experience a pretty horrible assessment and referral process. When I talk to school personnel, they tell me that, (a) they already know the students who are struggling, and (b) in year 2 of screenings, the rates of depression and suicidality plummet—because students are smart and they want to avoid the consequences of being open about their emotional state.
About 10-15% of people who complete suicide screenings feel worse afterward. We don’t really want that outcome.
There’s no evidence that school-based screenings are linked to reductions in suicide rates.
For more info on this, you can check out a brief commentary I published in the American Psychologist with my University of Montana colleague, Maegan Rides At The Door. The commentary focuses on suicide assessment with youth of color, but our points work for all youth. And, citations supporting our perspective are included.
Here are a few excerpts from the commentary:
Standardized questionnaires, although well-intended and sometimes helpful, can be emotionally activating and their use is not without risk (Bryan, 2022; de Beurs et al., 2016).
In their most recent recommendations, the United States Preventive Services Task Force (2022) concluded that the evidence supporting screening for suicide risk among children and adolescents was “insufficient” (p. 1534). Even screening proponents acknowledge, “There is currently little to no data to show that screening decreases suicide attempt or death rates” (Cwik et al., 2020, p. 255). . . . Across settings, little to no empirical evidence indicates that screening assessments provide accurate, predictive, or useful information for categorizing risk (Bryan, 2022).
I’ve got two events coming up, one sooner and one later.
This Friday, I’m doing the closing talk for Tamarack’s Grief Institute (which is on Thursday and Friday in Missoula, and available online too!).
This is late notice, as the end of day tomorrow (March 3) is the registration deadline. The whole Institute is worth attending. The fantastic Dr. Joyce Mphande-Finn kicks things off on Thursday morning. Then, the amazing Dr. Micki Burns takes over . . . and I’ll be bringing it home Friday afternoon. Check it out. Here’s a registration link:
This June, I have the incredible fortune of joining Dr. Jeff Linkenbach and the renowned Montana Summer Institute in Big Sky, Montana (and Livestream) from June 17-20. Here’s a description of what’s happening!
Reimagining Community Health:
Uncovering Positive Norms and & Activating Hidden
Protective Factors
In Big Sky, Montana and via Livestream: June 17-20, 2025
Join us at the 2025 Montana Summer Institute for three and a half transformative days dedicated to advancing community well-being. Through thought-provoking keynotes, interactive workshops, and engaging discussions, you’ll explore innovative strategies that leverage positive norms and amplify protective factors.
Learn to uncover hidden community strengths, identify untapped opportunities, and craft impactful communications that drive meaningful change. With insights from leading experts and experienced practitioners, you’ll gain practical tools to reimagine your approach to data, messaging, and the people you serve—all through a positive, effective frame.
Don’t miss this opportunity to expand your expertise, deepen your impact, and shape healthier, more resilient communities. For more information, visit www.montanainstitute.com
Is there any chance you will join us in June? It would be wonderful to have you there! Here is the Montana Discount Code to give $100 off the price: MSIMONT which would give $100 off registration
***********************
And here’s a fancy flyer for the Montana Summer Institute:
The following is an excerpt from a chapter I wrote with my colleagues Roni Johnson and Maegan Rides At The Door. The full chapter is in the Cambridge Handbook of Clinical Assessment and Diagnosis . . .
*********************************
The clinical interview is a fundamental assessment and intervention procedure that mental and behavioral health professionals learn and apply throughout their careers. Psychotherapists across all theoretical orientations, professional disciplines, and treatment settings employ different interviewing skills, including, but not limited to, nondirective listening, questioning, confrontation, interpretation, immediacy, and psychoeducation. As a process, the clinical interview functions as an assessment (e.g., neuropsychological or forensic examinations) or signals the initiation of counseling or psychotherapy. Either way, clinical interviewing involves formal or informal assessment. [For a short video on how to address client problems and goals in the clinical interview, see below]
Clinical interviewing is dynamic and flexible; every interview is a unique interpersonal interaction, with interviewers integrating cultural awareness, knowledge, and skills, as needed. It is difficult to imagine how clinicians could begin treatment without an initial clinical interview. In fact, clinicians who do not have competence in using clinical interviewing as a means to initiate and inform treatment would likely be considered unethical (Welfel, 2016).
Clinical interviewing has been defined as
“a complex and multidimensional interpersonal process that occurs between a professional service provider and client [or patient]. The primary goals are (1) assessment and (2) helping. To achieve these goals, individual clinicians may emphasize structured diagnostic questioning, spontaneous and collaborative talking and listening, or both. Clinicians use information obtained in an initial clinical interview to develop a [therapeutic relationship], case formulation, and treatment plan” (Sommers-Flanagan & Sommers-Flanagan, 2017, p. 6)
A Generic Clinical Interviewing Model
All clinical interviews follow a common process or outline. Shea (1998) offered a generic or atheoretical model, including five stages: (1) introduction, (2) opening, (3) body, (4) closing, and (5) termination. Each stage includes specific relational and technical tasks.
Introduction
The introduction stage begins at first contact. An introduction can occur via telephone, online, or when prospective clients read information about their therapist (e.g., online descriptions, informed consents, etc.). Client expectations, role induction, first impressions, and initial rapport-building are central issues and activities.
First impressions, whether developed through informed consent paperwork or initial greetings, can exert powerful influences on interview process and clinical outcomes. Mental health professionals who engage clients in ways that are respectful and culturally sensitive are likely to facilitate trust and collaboration, consequently resulting in more reliable and valid assessment data (Ganzini et al., 2013). Technical strategies include authentic opening statements that invite collaboration. For example, the clinician might say something like, “I’m looking forward to getting to know you better” and “I hope you’ll feel comfortable asking me whatever questions you like as we talk together today.” Using friendliness and small talk can be especially important to connecting with diverse clients (Hays, 2016; Sue & Sue, 2016). The introduction stage also includes discussions of (1) confidentiality, (2) therapist theoretical orientation, and (3) role induction (e.g., “Today I’ll be doing a diagnostic interview with you. That means I’ll be asking lots of questions. My goal is to better understand what’s been troubling you.”). The introduction ends when clinicians shift from paperwork and small talk to a focused inquiry into the client’s problems or goals.
Opening
The opening provides an initial focus. Most mental health practitioners begin clinical assessments by asking something like, “What concerns bring you to counseling today?” This question guides clients toward describing their presenting problem (i.e., psychiatrists refer to this as the “chief complaint”). Clinicians should be aware that opening with questions that are more social (e.g., “How are you today?” or “How was your week?”) prompt clients in ways that can unintentionally facilitate a less focused and more rambling opening stage. Similarly, beginning with direct questioning before establishing rapport and trust can elicit defensiveness and dissembling (Shea, 1998).
Many contemporary therapists prefer opening statements or questions with positive wording. For example, rather than asking about problems, therapists might ask, “What are your goals for our meeting today?” For clients with a diverse or minority identity, cultural adaptations may be needed to increase client comfort and make certain that opening questions are culturally appropriate and relevant. When focusing on diagnostic assessment and using a structured or semi-structured interview protocol, the formal opening statement may be scripted or geared toward obtaining an overview of potential psychiatric symptoms (e.g., “Does anyone in your family have a history of mental health problems?”; Tolin et al., 2018, p. 3).
Body
The interview purpose governs what happens during the body stage. If the purpose is to collect information pertaining to psychiatric diagnosis, the body includes diagnostic-focused questions. In contrast, if the purpose is to initiate psychotherapy, the focus could quickly turn toward the history of the problem and what specific behaviors, people, and experiences (including previous therapy) clients have found more or less helpful.
When the interview purpose is assessment, the body stage focuses on information gathering. Clinicians actively question clients about distressing symptoms, including their frequency, duration, intensity, and quality. During structured interviews, specific question protocols are followed. These protocols are designed to help clinicians stay focused and systematically collect reliable and valid assessment data.
Closing
As the interview progresses, it is the clinician’s responsibility to organize and close the session in ways that assure there is adequate time to accomplish the primary interview goals. Tasks and activities linked to the closing include (1) providing support and reassurance for clients, (2) returning to role induction and client expectations, (3) summarizing crucial themes and issues, (4) providing an early case formulation or mental disorder diagnosis, (5) instilling hope, and, as needed, (6) focusing on future homework, future sessions, and scheduling (Sommers-Flanagan & Sommers-Flanagan, 2017).
Termination
Termination involves ending the session and parting ways. The termination stage requires excellent time management skills; it also requires intentional sensitivity and responsiveness to how clients might react to endings in general or leaving the therapy office in particular. Dealing with termination can be challenging. Often, at the end of an initial session, clinicians will not have enough information to establish a diagnosis. When diagnostic uncertainty exists, clinicians may need to continue gathering information about client symptoms during a second or third session. Including collateral informants to triangulate diagnostic information may be useful or necessary.
See the 7th edition of Clinical Interviewing for MUCH more on this topic:
This post is for my Chinese friends, or my friends who speak Mandarin . . . or anyone who wants to read about the process of self-evaluation, the pain of self-reflection, and personal/professional growth.
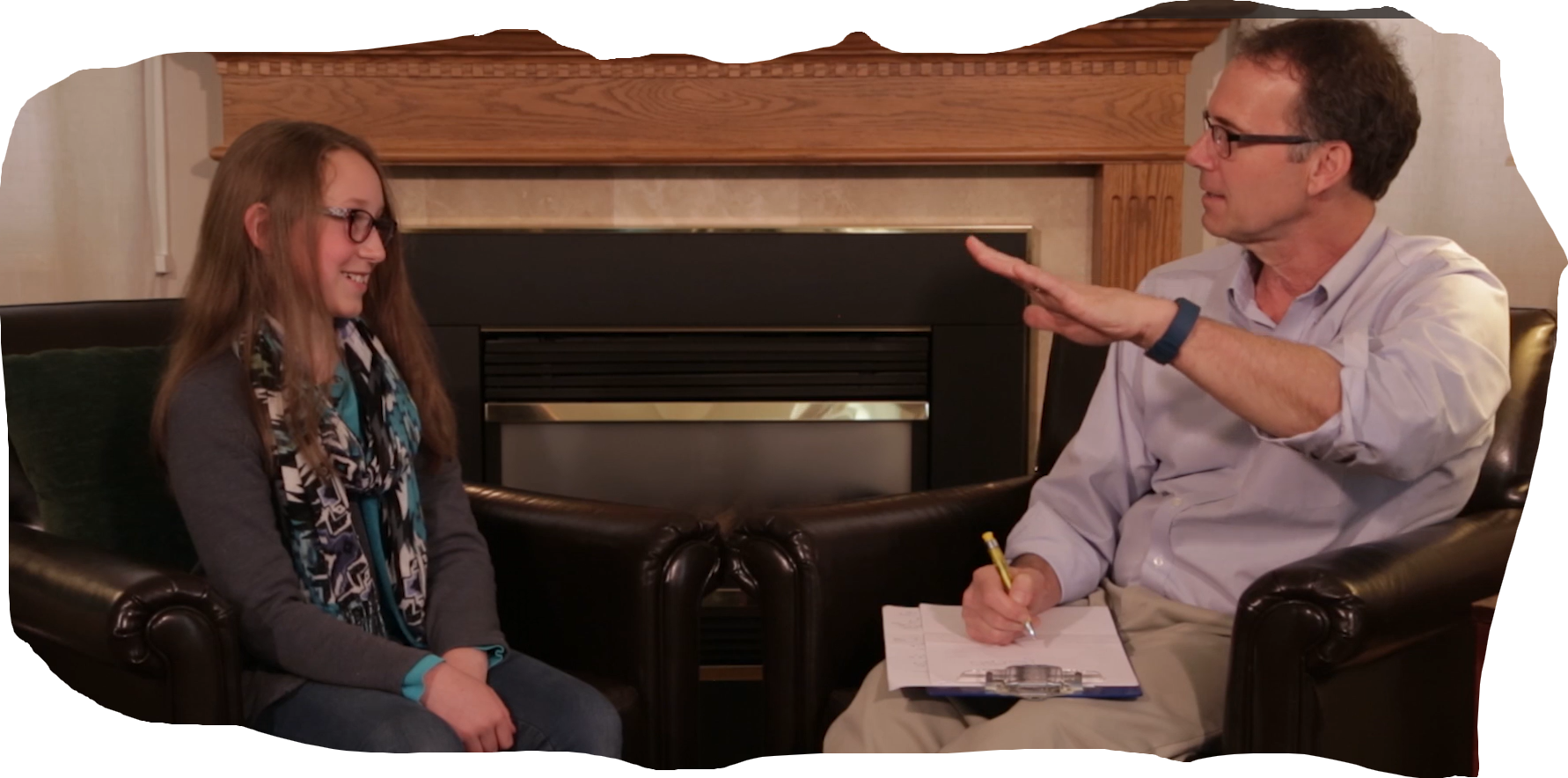
Last year I was asked to participate as a psychotherapist for the One-Way Mirror Project. The project was inspired by the old and now classic “Three Approaches to Psychotherapy” videos. Not surprisingly, I was honored to be asked to participate, and said yes despite a number of challenging factors, including doing therapy late at night with a Chinese woman via Zoom. I share this because this post is about transparency and so I’m transparently beginning by making excuses for not being the best therapist I imagine myself to be.
Here’s the scenario: One session. Minimal pre-meeting information. Post-session viewing (by me) and commentary on my performance. One other therapist also met with the same client. I get to watch his session; he gets to watch mine. We then have a Zoom meeting to debrief and share our thoughts about our respective sessions (mine was in English; his was in Mandarin).
This was a super-interesting process.
Below, I’m sharing my written self-reflection comments. There’s also a video version . . . which is similar to, but not verbatim from, these notes. The comments are numbered sequentially.
I hope you enjoy this self-reflection/analysis. Thanks for reading.
John S-F – Commentary on His Session with Evelyn
My first reaction to watching this video of myself was embarrassment. I’m sharing this reaction because it’s true. I don’t want to pretend that I think this is a particularly good session.
That said, I also don’t think it was a particularly bad session. I did some things well, and some things less well. In this commentary I will try to describe: (a) what I’m doing (or trying to do), especially from different theoretical perspectives, (b) how Evelyn is responding, (c) what I’m doing well and what I’m doing that’s much less good.
In critiquing my own work, I’m also hoping to connect with all of you. Whether you’re a beginning student or an experienced professional psychotherapist, watching ourselves and hearing ourselves can be humbling and embarrassing. It’s natural for all of us to make mistakes and be imperfect . . . and in this session I do an excellent job of being imperfect😊. . . so much so that while watching the video, during several points I kept shouting at myself to “shut up!” So, that’s a glimpse into one thing I would change about MY behavior in this session. Although I’m okay with being imperfect, I’m not very comfortable with being as imperfect as I was in this session.
How I Work – 0:10 – This explanation has three main goals. First, I’m showing transparency, which is consistent with person-centered and feminist therapies. Second, I’m explaining the process of our session, which is a role induction designed to help clarify expectations. Third, I’m including an invitation for collaboration.
SFBT Opening Question – 1:30 – “If we have a useful meeting, what will we accomplish?” This is a goal-oriented question to help me be more aware of Evelyn’s vision of a successful session.
Evelyn’s Goal – 1:50 – Evelyn says she wants a “different perspective” of what she’s worried about.
JSF’s Goal – In a single session treatment, and maybe most therapy sessions, it’s best to begin with what the client wants. Evelyn’s goal is a “cognitive goal.” In this moment, I decide to go with George Kelly’s “Credulous approach to assessment,” which essentially means “believe the client.” That could be a variation of Carl Rogers’s assertion that we should “Trust the client, because the client knows what hurts and where to go.” JSF – Your goal is my goal, as long as it’s legal and healthy.”
What I Know – 2:25 – This is another effort to be like Carl Rogers and show transparency.
Feelings and Thoughts Around That – 3:00 – Here, I’m trying to prompt her to explore feelings and/or thoughts. She says, “So many worries overwhelming” and talks about not knowing what is overwhelming and then references social media, and four main issues/worries: (a) Fitness/body image/comparison, (b) feelings of unfairness related to gender issues, (c) she loves her partner, but “he is a man” (with sarcasm, implying he therefore cannot understand), (d) humiliation linked to breasts filling with milk involuntarily.
A Broad Summary/Paraphrase – I respond with an accurate summary of her four “feelings and thoughts”
“You can choose; I cannot” – 7:10 – Evelyn focuses on the inherent sex/gender unfairness as related to having a baby. In response, we discuss the burden of social responsibility and how she has internalized societal expectations around being a woman.
May I Share an Observation? – 8:30 – At this point, I try to be a mirror that reflects back to Evelyn what I’m experiencing as one of her positive attributes or strengths. When working across cultures, it’s especially important to be affirming of client strengths. I end this reflection using first-person pronouns—which is a language skill that Rogers used and called “Walking within” – 9:10
Evelyn Continues – 10:45 – to talk about feeling powerless and influenced by her age, generation, societal expectations, and then notes that she wants to “make peace with what she wants to be and what she can be.” The thought of having a baby is a particular trigger for her anxious thoughts and fears. – 11:15
An Intellectual Grasp – 12:15 – I observe that Evelyn has a good intellectual grasp of feminism and of her internalized expectations about how women should be.
A Reflection and SFBT Question – 12:35–13:29 – Using too many words, I finally get out a “Unique outcomes” question: “How have you dealt with internalized fears and conflicts before?”
I Love That Question – 13:35 – Evelyn reflects on a story from age 24 and provides examples of how she felt time running out, dated like crazy, was very brave, and fought back toward her goal of a loving relationship even after having her heart broken.
How did you manage? – 15:03 – I continue to pursue Evelyn’s pre-existing strengths and insights around, with a bit of a focus on what motivated her to “fight back.”
As a Good Therapist – 15:35 – Evelyn expresses motivation to be a good therapist and that requires expansive live experiences.
Anything Else Pull You – 16:54 – Evelyn shares an early fear of death, noting, after an anecdote, that her class presentation on death left her feeling “more lonely (or different) than ever.” – 17:54. [not psychoanalytic]
I Reflect – 18:30 – Being a better therapist and fear of death motivate her to live a life full of experiences.
Imagine self at end of life – 19:00 – Found someone I love and would like to have a child. I want to try it. That would complete my experience. – 19:30
Values vs. Anxieties – 19:55 – Still feel anxieties. “I have to carry a child” etc. . . walking within. Amplifying expectations so she can hear them.
That’s my barrier –
Fought those off those expectations before – 20:45 – And yet . . . you have fought off expectations before. What makes you think you will be a victim to those expectations in the future? Here, I’m trying to identify what CBT people might consider an “irrational” or “maladaptive” thought/belief that doesn’t have much evidence to support it. Also, exception. . .
Focus on the Physical/Somatic – 22:25 – Evelyn notes this task is “harder” and supports that with physical changes she’s experiencing with aging. . . and I interpret that as “Anticipatory grief” regarding her physical decline [this is likely death anxiety too]
Self-Disclosure – 23:40 – May I share something? “I have a 35-y/o daughter with similar issues.” [Too many words! Should have stopped when Evelyn laughed and put her hand to her face and then explored her initial reaction]. I finally get to “What’s your reaction?” [Late, but I got there]. She says . . . and this is potentially central to “one” therapy goal: “I feel, like, less lonely.” [Again, I should just stop there or repeat it back. . . or “What’s it like inside to feel less lonely?”].
Curious about what I could learn from her – 25:35 – I turn this around. Why? Because I want her to value herself as a source of wisdom.
When I share with my partner – 26:25 – She notes “he can relate” and that “men are limited.” [This could have been good transference exploration or Adlerian basic mistake]
Session shift to “so much feeling” – 27:16 – Evelyn is talking about her emotionality, I’m reflecting ok. More on unfairness, but notes BF is pretty accepting. I do a strength-based reflection, “Openness, strength, do not run from feelings!” This is a little CBT as I want her to “perceive” herself with more strengths to cope with her future challenges.
Thoughts about yourself? – 31:00 – I’ve been working on some CBT stuff and now am shifting back to the important self-evaluation process. Her response is constructive as she describes lots of planning she has already done for this coming year.
I want to hear out my fears – 32:10 – This is a great insight on her part. It prompts me to have her listen to her fears in the here and now. Evelyn responds [33:10] that she likes that question and explores, perhaps with a tiny bit of surprise, that her fears are not harsh, but more of a gentle reminder to not have regrets. [Here, I could and probably should have had her get deeper into here and now processing. “Let’s have you hear the gentle voice of your fear right now. What’s it saying to you? Say it as if you are the fear. Also, could have used repetition.]
Reflections and WW – I stay with the themes and use WW to keep bringing them back. Why? In part, desensitization. Hearing her anxiety-producing words in a potentially trusting/comforting setting can take some edge or power out of them [MCJ – 1924]. She says, somewhat conclusively, “Sounds like fear just wants me to get prepared and not critique.” [One thought, I could have been her child and asked her to tell me what she has learned.]
Evelyn asks JSF Q – 36:28 – This is one place where I fall off the rails. She asked me a question and my obnoxious, intellectual, professor-self emerges. . . for far too long. [I could have said, “I have some thoughts about that, but I’d like to hear yours first.”] Instead, JSF blah, blah, blah, and to compound the error, I do not check in on her reaction.
Evelyn continues exploring – 40:52 – She notes Yuval Harrare and feminism as a new way to resolve conflicts without war. I do manage to shift back to listening with a pretty good paraphrase: “Communication with your partner may be your best way to grow and develop and maintain your feminist identity through childbirth and your relationship.”
Evelyn recognizes perfect equality not possible – 42:35 – JSF “Love what you said. What do you think? How does it feel?” [2 Qs, boo, but my focus on her self-evaluation is still pretty solid.] I continue with “What’s your assessment of yourself and your communication skills?” I’m hoping she can express trust in her communication skills.
Non-violent communication as restraint – 46:00 – This is an interesting side road where E says, “Sometimes I just want to be violent and like a child” and notes that she prefers “emotionally charged communication.” She finds emotions and aggressive communication to be helpful. [Note: at this point I’m beginning to feel time pressure. No time to go deeper. If more sessions, I’d earmark this and close. Instead, I ask, “Is it ok to have both” (nonviolent and emotional communication) as a quick prompt toward integration.
Moving toward closing – 49:00 – I’ve lost track of time because of early tech problems. I’d like to think that’s my excuse for ending poorly. First, I begin a summary. This isn’t good. It’s MY summary . . . and I should be asking for HER summary before offering mine. I’m far too verbal. The content isn’t terrible.
Thank-you so much – 52:45 – She’s tracking time, and this should be it. I’m not. And do another disclosure and ask for her summary.
Sorry for all the posts, but apparently there’s lots happening in early 2025.
The big NEWS post won’t be until tomorrow.
As you know, on this Friday, January 10, I’ll be doing an online, two-hour workshop on Strategies for Integrating Traditional and Strengths-Based Approaches to Suicide for the Cognitive Behavior Institute.
I’m posting the workshop handouts here, in advance, for anyone interested.
Last week I shared my 2025 predictions with you. This week, I’ve got another prediction . On Friday, January 10, I’ll be doing an online, two-hour workshop (title listed above) for the Cognitive Behavior Institute. I predict that if you sign up, you’ll be happy you did.
The other good news about this workshop is that it’s ALMOST FREE. Only $25. Here’s the link to register:
If you’re interested in this topic and can’t make it (or even if you can make it), here’s a pdf of an article I wrote about suicide assessment for a Psych journal in 2018:
Every day, I keep getting older. I can’t seem to stop myself. And every day, I keep running into dialectics. They’re everywhere. My aging experiences of ubiquitous dialectics seems consistent with the fact that yesterday, Merriam-Webster declared “polarization” their word of the year (https://www.merriam-webster.com/wordplay/word-of-the-year).
Boo, Merriam-Webster! I would have chosen dialectics. Here’s one of the definitions for dialectic listed in the online M-W dictionary: “the Hegelian process of change in which a concept or its realization passes over into and is preserved and fulfilled by its opposite.” TBH, I have very little understanding of what the heck Hegel was talking about, but I’m pretty sure it’s happening ALL. THE. TIME.
This morning I find myself plagued by the idea that although most mental health professionals advocate mindfulness, many mental health professionals (including myself, sometimes), aren’t very mindful when using basic counseling skills in practice. Today’s topic is questions. I’m polarized inside a dialectical and thinking, “We should all be more mindful and intentional in our use of questions in counseling and psychotherapy.” At the same time, I’m sure, “we should all relax and be more of ourselves.”
With these confusing caveats in mind, today, tomorrow, and maybe the next day, I’m posting about the very basic use of questions in counseling and psychotherapy. This content is excerpted from our Clinical Interviewing textbook.
Here’s our opening section on questions, which is conveniently found in Chapter 5 of Clinical Interviewing, which I’m continually surprised that not everyone has read (but really not at all surprised).
**************************************
Questions
Imagine digging a hole without a shovel or building a house without a hammer. For many clinicians, conducting an interview without using questions constitutes an analogous problem: How can you complete the interviewing task without using your most basic tool?
Despite the central role of questions in clinical interviewing, we’ve avoided discussing them until now. Similarly, when teaching clinical interviewing skills, we usually prohibit question asking for a significant portion of the course (J. Sommers-Flanagan & Means, 1987). Our rationale includes several factors: Questions are easy and often misused. Also, because questioning isn’t the same thing as listening, our goal is for students to develop alternative information-gathering strategies. Asking questions can get in the way of gathering important information from clients. The Little Prince expresses a fundamental problem with excessive questioning.
Grown-ups love figures. When you tell them that you have made a new friend, they never ask you any questions about essential matters. They never say to you, “What does his voice sound like? What games does he love best? Does he collect butterflies?” Instead, they demand: “How old is he? How many brothers has he? How much does he weigh? How much money does his father make?” Only from these figures do they think they have learned anything about him. (de Saint-Exupéry, 1943/1971, p. 17)
The questions you ask may be of no value to the person being asked. Ideally, your questions should focus on what seems most important to clients.
Despite our reservations about excessive questioning, questions are a diverse and flexible interviewing tool; they can be used to
Stimulate client talk
Inhibit client talk
Facilitate rapport
Show interest in clients
Show disinterest in clients
Gather information
Confront clients
Focus on solutions
Ignore the client’s viewpoint
Stimulate insight
There are many forms or types of questions. Differentiating among them is important, because different question types produce different client responses. In this section, we describe open, closed, swing, indirect, and projective questions. Chapter 6 covers therapeutic questions. Although we distinguish between general question types and therapeutic questions, all questioning can be used for assessment or therapeutic purposes.
Open Questions
Open questions are used to facilitate talk; they pull for more than a single-word response. Open questions ordinarily begin with either How or What. Sometimes questions that begin with Where, When, Why, and/or Who are classified as open, but such questions are only partially open because they don’t facilitate talk as well as How and What questions (Cormier, Nurius, & Osborn, 2017). The following hypothetical dialogue illustrates how using open questions may or may not stimulate client talk:
Therapist: When did you first begin having panic attacks?
Client: In 1996.
Therapist: Where were you when you had your first panic attack?
Client: I was just getting on the subway in New York City.
Therapist: Why haven’t you tried to ride the subway again?
Client: Because I’m afraid I’ll have another panic attack.
Therapist: How are you handling the fact that your fear of panic attacks is so restrictive?
Client: Not so good. I’ve been getting more and more scared to go out. I’m afraid that soon I’ll be too scared to leave my house.
As you can see from this example, open questions vary in their openness. They don’t uniformly facilitate depth and breadth of talk. Although questions beginning with What or How usually elicit the most elaborate responses from clients, that’s not always the case. More often, what’s important is the way a particular What or How question is phrased. For example, “What time did you get home?” and “How are you feeling?” can be answered very succinctly. The openness of a particular question should be judged primarily by the response it usually elicits.
Questions beginning with Why are unique in that they commonly elicit defensive explanations. Meier and Davis (2020) wrote, “Questions, particularly ‘why’ questions, put clients on the defensive and ask them to explain their behavior” (p. 23). Why questions frequently produce one of two responses. First, as in the preceding example, clients may respond with a form of “Because!” and then explain, sometimes through detailed and intellectual responses, why they’re thinking or acting or feeling in a particular manner. Second, some clients defend themselves with a “Why not?” response. Or, because they feel attacked, they respond confrontationally with “Is there anything wrong with that?” Therapists minimize Why questions because they exacerbate defensiveness and intellectualization and diminish rapport. In contrast, if rapport is good and you want your client to move away from emotions and speculate or intellectualize about something, then a Why question may be appropriate and useful.
Closed Questions
Closed questions usually begin with words such as Do, Does, Did, Is, Was, or Are and can be answered with a yes or no response. They’re useful if you want to solicit specific information. Traditionally, closed questions are used later in the interview, when rapport is established, time is short, and efficient questions and short responses are needed (Morrison, 2007). Questions that begin with Who, Where, or When also tend to direct clients toward talking about specific information; therefore, they should be considered closed questions (see Practice and Reflection 5.1).
Closed questions restrict verbalization and lead clients toward details. They can reduce or control how much clients talk. Restricting verbal output is useful when working with clients who talk excessively. Closed questions are used to clarify behaviors and symptoms and consequently used when conducting diagnostic interviews. (For example, in the preceding example about a panic attack on the New York subway, a diagnostic interviewer might ask, “Did you feel lightheaded or dizzy?” This question would help confirm or disconfirm one symptom possibly linked to panic disorder.). As compared to open questions, closed questions usually feel different to clients.
Sometimes, therapists inadvertently or intentionally transform open questions into closed questions with what’s called a tag query. For example, you might start with, “What was it like for you to confront your father after all these years,” and then tag “was it gratifying?” onto the end.
Transforming open questions into closed questions is fine if you want to limit client elaboration. When asked closed question, clients will likely focus solely on the answer (e.g., whether they felt gratification when confronting their father, as in the preceding example). Clients may or may not elaborate on feelings of fear, relief, resentment, or other thoughts, emotions, and sensations.
If you begin an interview using a nondirective approach, but later change styles to obtain more specific information through closed questions, it’s wise to use role induction to inform your client of your forthcoming shift. You might say,
We have about 15 minutes left, and I have a few things I want to make sure I’ve covered, so I’m going to start asking you more specific questions.
Beginning therapists are usually advised to avoid closed questions because closed questions are frequently interpreted as veiled suggestions. For example:
Client: Ever since my husband came back from active duty, he’s been moody, irritable, and withdrawn. This makes me miss him terribly, even though he’s home. I just want my old husband back.
Therapist: Have you tried telling him how you’re feeling?
We usually boldly tell our students to never ask, “Have you tried. . .” We believe have you questions are advice-giving in disguise. We’re not against advice; we’re just against asking questions that imply clients should have already tried what you’re recommending. In the preceding interaction, the client might think the therapist is suggesting she should open up to her husband about her feelings. Although this may be a reasonable idea, therapists and clients are better served with an open question: “What have you tried to help get your old husband back?” Our advice—which is not disguised in the least—is that when you feel an impulse to ask a “have you” question (and you will), simply stop yourself, and add the word “What” to the beginning to make it an open question. Closed questions are a helpful interviewing tool—as long as they’re used intentionally and in ways consistent with their purpose.
Swing Questions
Swing questions can function as either closed or open questions; they can be answered with yes or no, but they also invite more elaborate discussion of feelings, thoughts, or issues (Shea, 1998). Swing questions usually begin with Could, Would, Can, or Will. For example:
Could you talk about how it was when you first discovered you were pregnant?
Would you describe how you think your parents might react to finding out you’re leaving?
Can you tell me more about that?
Will you tell me what happened in the argument between you and your daughter last night?
Ivey and colleagues (2023) believe swing questions are the most open of all questions. They note that clients are empowered to decline answering a swing question by saying something like, “No. I’d rather not talk about that.”
For swing questions to work, you should observe two basic rules. First, avoid using swing questions unless rapport has been established. Without rapport, swing questions may backfire and function as a closed question (i.e., the client responds with a shy or resistant yes or no). Second, avoid using swing questions with children and adolescents, especially early in the relationship. This is because children and adolescents often interpret swing questions concretely and respond accordingly (J. Sommers-Flanagan & Sommers-Flanagan, 2007b). For example:
Counselor 1: Would you tell me more about the fights you’ve been having with your classmates?
Young Client 1: No.
Counselor 2: Could you tell me about how you felt when your dad left?
Young Client 2: No.
Counselor 3: Would you like to come back to my office?
Young Client 3: No.
Swing questions with young clients (especially if you don’t have positive rapport) can produce awkward and unhelpful interactions.
Indirect or Implied Questions
Indirect or implied questions usually begin with I wonder or You must or It must (Benjamin, 1987). They’re used when therapists don’t want to directly ask or pressure clients to respond. The following are examples of indirect or implied questions:
I wonder how you’re feeling about your upcoming wedding.
I’m wondering about your plans after graduation.
I’m curious if you’ve given any thought to searching for a job.
You must have some thoughts or feelings about discovering your child is transgender.
It must be hard for you to cope with your wife being shipped out to serve overseas.
You can use other indirect sentence stems to gently imply a question or prompt clients to speak about a topic. Common examples include “I’d like to hear about…” and “Tell me about…”
Indirect or implied questions can be useful early in interviews or when approaching delicate topics. Like immediacy, they can contain a supportive self-disclosure of interest. They’re noncoercive, so they may be especially useful as an alternative to direct questions with clients who seem reticent (C. Luke, personal communication, August 7, 2012). When overused, indirect questions can seem sneaky or manipulative; after repeated “I wonder…” and “You must…” probes, clients may start thinking, “And I’m wondering why you don’t just ask me whatever it is you want know!”
Projective or Presuppositional Questions
Projective questions are used to ask clients to imagine particular scenarios and help them identify, explore, and clarify unconscious or unarticulated conflicts, values, thoughts, and feelings (see Case Example 5.5). Solution-focused therapists refer to projective questions as presuppositional questions (Murphy, 2023). These questions typically begin with some form of What if and invite client speculation. Projective questions can trigger mental imagery and prompt clients to explore thoughts, feelings, and behaviors they might have if they were in a particular situation. For example:
What would you do if you were given one million dollars?
If you had three wishes, what would you wish for?
If you needed help or were really frightened, or even if you were just totally out of money and needed some, who would you turn to right now? (J. Sommers-Flanagan & Sommers-Flanagan, 1998, p. 193)
What if you could go back and change how you acted during that argument (or other significant life event): What would you do differently?
Projective questions are also used to evaluate client values, decision making, and judgment. For example, a therapist can analyze a response to the question “What would you do with one million dollars?” to glimpse client values and self-control. Projective questions are sometimes included as a part of mental status examinations (see Chapter 9 and the Appendix).
CASE EXAMPLE 5.5: PROJECTIVE QUESTIONING TO ELICIT VALUES
Your use of projective questions is limited only by your creativity. John likes to use projective questions to explore relationship dynamics and values. For example, with a 15-year-old male client who had an estranged relationship with his father and was struggling in school, John asked, “If you did really well on a test, who’s the first person you would tell?” The client responded, “My dad.” After hearing this response, John used the fact that the boy continued to value his father’s approval to encourage the boy and his father to meet together for counseling to improve their communication and relationship.
[End of Case Example 5.5]
And . . . here’s a pdf of the Chapter 5 Table describing the different question types.
Tomorrow, December 4, I’m doing a quick one-hour version of my “Integration” workshop. Obviously, my leaning is toward the strengths-based, constructive approach to suicide assessment and treatment, but sometimes we need to integrate strengths-based approaches with the traditional medical model. That’s what this workshop is all about.
The workshop is presented on behalf of the Professional Counseling Association of Montana — the brainchild of Cynthia Boyle, a Ph.D. student in the University of Montana’s counseling and supervision program. Here’s a link to their website: https://pcamontana.org/
In case you’re attending . . . or interested . . . here are the slides:
[I love the preceding photo because I’m doing a workshop on suicide in Billings, Montana, and despite the content, the participants are clearly having a good time]
Sometimes people ask me if I have presentations coming up. Other times they ask me about recent presentations. For reasons related to my own inability to be more organized and behave responsibly, I haven’t been very good at inserting “upcoming events” into my schedule, or at sharing links with readers about recent content that’s available online. Today’s post is my effort to address my irresponsibility.
September 11, 2024 – JSF presented a day-long ONLINE workshop, Conducting Parenting Consultations on behalf of Families First. Missoula, MT. Here are the ppts for the Parenting Consultation workshop:
September 26, 2024 – JSF presented a day-long IN-PERSON workshop, Tough Kids, Cool Counseling on behalf of Families First. Missoula, MT.
October 10, 2024 – JSF presented a day-long IN-PERSON workshop, Strengths-Based Suicide Assessment and Treatment on behalf of Tribal Health, Ronan, MT.
October 24, 2024 – JSF did an on-air guest interview on Evidence-Based Happiness for Teachers on a South Korean radio station. https://youtu.be/xYdJOInpAkE
November 6, 2024 – JSF presented on Let’s Pursue Happiness . . . Together (with our children) to the Washington Middle School Parent Teacher Association (PTA)
November 7, 2024 – JSF presented IN-PERSON on Why We Should Be in Pursuit of Eudaimonia (Not “Happiness”) for the University of Montana Alumni Association. Missoula, MT.
UPCOMING ACTIVITIES AND EVENTS
November 13 – JSF is presenting Let’s Pursue Happiness Together [In our schools . . . with our teachers . . . and for our children]ONLINE to the Montana Office of Public Instruction Montana Student Wellness Advisory Committee.
November 14 – JSF is presenting Happiness and You: Methods for Managing Your MoodsIN PERSON at the annual statewide Future Farmers of America (FFA) conference at MSU in Bozeman, MT.
December 4 – JSF is presenting a one-hour workshop on Strengths-Based Integrating Strengths-Based and Traditional (Medical Model) Approaches to Suicide AssessmentONLINE to the Professional Counseling Association of Montana. Link unavailable for now.
December 6 John Sommers-Flanagan is presenting an all-day ONLINE workshop for mental health professionals titled, Tough Kids, Cool Counseling, on behalf of the Vermont Psychological Association. Info is here: https://twinstates.ce21.com/speaker/john-sommersflanagan-2295709
January 10 – JSF is doing a 2-hour ONLINE workshop titled, Strategies for Integrating Traditional and Strengths-Based Approaches to Suicide, through the Cognitive Behavior Institute. You can register here for $25.00: https://www.pathlms.com/cbi/courses/77936#
The place to click if you want to learn about psychotherapy, counseling, or whatever John SF is thinking about.