Every chapter in Clinical Interviewing has several pop-out boxes titled, “Practice and Reflection.” In this–the latest–edition, we added many that include the practice and perspective of diverse counselors and psychotherapists. Here’s an example from Chapter One.
PRACTICE AND REFLECTION 1.3: AM I A GOOD FIT? NAVIGATING ETHNIC MATCHING IN PRIVATE PRACTICE
The effects of ethnic matching on counseling outcomes is mixed. In some cases and settings, and with some individuals, ethnic matching improves treatment frequency, duration, and outcomes; in other cases and settings, ethnic matching appears to have no effects in either direction (Olaniyan et al., 2022; Stice et al., 2021). Overall, counseling with someone who is an ethnic/cultural match is meaningful for some clients, while other clients obtain equal meaning and positive outcomes working with culturally different therapists.
For clients who want to work with therapists who have similar backgrounds and experiences, the availability of ethnically-diverse therapists is required. In the essay below, Galana Chookolingo, Ph.D., HSP-P, a licensed psychologist, writes of personal and professional experiences as a South Asian person in independent practice.
On a personal note, being from a South Asian background in private practice has placed me in a position to connect with other Asians/South Asians in need of culturally-competent counseling. In my two years in solo private practice, I have had many individuals reach out to me specifically because of my ethnicity and/or the fact that I am also an immigrant to the U.S. (which I openly share on my website). These individuals hold an assumption that I would be able to relate to a more collectivistic worldview. Because I offer free consultations prior to meeting with clients for an intake, I have had several clients ask directly about my ability to understand certain family dynamics inherent to Asian cultures. I have responded openly to these questions, sharing the similarities and differences I am aware of, as well as my limitations, since I moved to the U.S. before age 10. For the most part, I have been able to connect with many clients of Asian backgrounds; this tends to be the majority of my caseload at any given time.
As you enter into the multicultural domain of counseling and psychotherapy, reflect on your ethnic, cultural, gender, sexual, religious, and ability identities. As a client, would you prefer working with someone with a background or identity similar to yours? What might be the benefits? Alternatively, as a client, might there be situations when you would prefer working with someone who has a background/identity different than yours? If so, why and why not?
Reflecting on Dr. Chookolingo’s success in attracting and working with other Asian/South Asian people . . . what specific actions did she take to build her caseload? How did she achieve her success?
[End of Practice and Reflection 1.3]
For more info on ethnic matching, see these articles:
Olaniyan, F., & Hayes, G. (2022). Just ethnic matching? Racial and ethnic minority students and culturally appropriate mental health provision at British universities. International Journal of Qualitative Studies on Health and Well-being, 17(1), 16. doi:https://doi.org/10.1080/17482631.2022.2117444
Stice, E., Onipede, Z. A., Shaw, H., Rohde, P., & Gau, J. M. (2021). Effectiveness of the body project eating disorder prevention program for different racial and ethnic groups and an evaluation of the potential benefits of ethnic matching. Journal of Consulting and Clinical Psychology, 89(12), 1007-1019. doi:https://doi.org/10.1037/ccp0000697
Irritability is a fascinating experience. It’s hard to perfectly describe, so I looked up the definition online. Dictionary says: “The quality or state of being irritable.” Hahaha. This is the sort of helpfulness I’ve been experiencing from the pesky universe lately. . . with the exception of the IT guy who helped me for 45 minutes a couple weeks ago. He was nice and tried to help, but sadly, I’m the guy who was once told by IT person at UM that maybe I had swallowed a magnet because of how well electronics work in my presence. Maybe it’s my magnetic personality? Even more hahaha.
Let’s get back to irritability. Lately, I’ve been beset with intermittent bouts of irritability, which, I understand is the quality or state of being irritable. The definition of irritable is more illuminating: “having or showing a tendency to be easily annoyed or made angry.”
Yes, I’ve got that. In my defense, there are SO MANY irritating things in the world.
But there’s really no good excuse for my irritability. I feel it burble up, usually in response to something psychologically, emotionally, or physically painful. I’ve had some chronic pain for the past three months, which makes it easier for my irritability button to get pushed. I’ve also had more than my share of tech problems.
After working out at the gym, a particular Dean whom I saw on campus, asked me, “Did you have a good workout?” I muttered something about never having good workouts anymore. Not surprisingly, he noticed my irritability. Then he shared a few Buddhist thoughts about “All is suffering” with me. Despite my internal lean toward being “easily annoyed” (even with my friend the Dean) I listened and immediately glimpsed my lifelong nemesis peeking at me from around the corner. No . . . it wasn’t the Dean, or Lee Jeffries the red-headed bully who tormented me in junior high. Strangely, my lifelong nemesis happens to be the nemesis of many. I’m betting it may be yours as well.
Given that our nemesis has multitudes, let’s give it the pronoun they. They have a name. Expectations.
My expectations are routinely laughably unrealistic. I know that about myself. I also know that when I set myself up with expectations for an hour or a day, the hour or the day includes more irritability. My friend the Dean was commenting on the All-American tendency to expect happiness, whereas the Buddhists embrace that “all is suffering.”
Several weeks ago, the focus of the Happiness Challenge was on goal-setting. I didn’t do much goal-setting back then, which is okay, because goal-setting should happen when we’re ready for goal-setting. I also know that this week’s Happiness Challenge is about cognitive behavior therapy (CBT). And so this week I’ve been working on a goal to be more immediately self-aware of my expectations and irritability triggers, and to make a concerted effort to manage my irritability in ways I feel good about.
To enhance my self-awareness, I completed the “column technique” for myself and my relationship with irritability. Although I’m not a natural fan of CBT, I found the process helpful, if not illuminating. What was most helpful was to fill out the columns—like a journal—and then read through what I had written. My response was to feel a little embarrassed at the triviality of my irritability triggers. And . . . as Alfred Adler wrote about a century ago, insight (aka self-awareness) is a natural motivator.
For anyone interested, here’s my completed column log activity.
In the end, glimpsing my process and experiences through the column technique this week has made me more motivated that ever to address my irritability in a positive and constructive way.
This morning’s weekly missive of “most read” articles from the Journal of the American Medical Association included a study evaluating the effects of high-dose “fluvoxamine and time to sustained recover in outpatients with COVID-19.” My reaction to the title was puzzlement. What could be the rationale for using a serotonin specific reuptake inhibitor for treating COVID-19? I read a bit and discovered there’s an idea and observations that perhaps fluvoxamine can reduce the inflammation response and prevention development of more severe COVID-19.
To summarize, the results were no results. Despite the fact that back in the 1990s some psychiatrists and pharmaceutical companies were campaigning for putting serotonin in the water systems, in fact, serotonin doesn’t really do much. As you know from last week, serotonin-based medications are generally less effective for depression than exercise.
For the happiness challenge this week, we’re touting the effectiveness of my own version of what we should put in the water or in the schools or in families—the Three-Step Emotional Change Trick. Having been in a several month funk over a variety of issues, I find myself returning to the application of the Three-Step Emotional Change Trick in my daily life. Does it always work? Nope. Is it better than feeling like a victim to my unpleasant thoughts and feelings? Yep.
I hope you’ll try this out and follow the instructions to push the process outward by sharing and teaching the three steps. Let’s try to get it into the water system.
Active Learning Assignment 9 – The 3-Step Emotional Change Trick
Almost no one likes toxic positivity. . . which is why I want to emphasize from the start, this week’s activity is NOT toxic positivity.
Back in the 1990s I was in full-time private practice and mostly I got young client referrals. When they entered my office, nearly all the youth were in bad moods. They were unhappy, sad, anxious, angry, and usually unpleasantly irritable. Early on I realized I had to do something to help them change their moods.
An Adlerian psychologist, Harold Mosak, had researched the emotional pushbutton technique. I turned it into a simple, three-step emotional change technique to help young clients deal with their bad moods. I liked the technique so well that I did it in my office, with myself, with parents, during professional workshops, and with classrooms full of elementary, middle, and high school students. Mostly it worked. Sometimes it didn’t.
This week, your assignment is to apply the three-step emotional change trick to yourself and your life. Here’s how it goes.
Introduction
Bad moods are normal. I would ask young clients, “Have you ever been in a bad mood?” All the kids nodded, flipped me off, or said things like, “No duh.”
Then I’d ask, “Have you ever had somebody tell you to cheer up?” Everyone said, “Yes!” and told me how much they hated being told to cheer up. I would agree and commiserate with them on how ridiculous it was for anyone to ever think that saying “Cheer up” would do anything but piss the person off even more. I’d say, “I’ll never tell you to cheer up.* If you’re in a bad mood, I figure you’ve got a good reason to be in a bad mood, and so I’ll just respect your mood.” [*Note to Therapists: This might be the single-most important therapeutic statement in this whole process.]
Then I’d ask. “Have you ever been stuck in a bad mood and have it last longer than you wanted it to?”
Nearly always there was a head nod; I’d join in and admit to the same. “Damn those bad moods. Sometimes they last and last and hang around way longer than they need to. How about I teach you this thing I call the three-step emotional change trick. It’s a way to change your mood, but only when YOU want to change your mood. You get to be the captain of your own emotional ship.”
Emotions are universally challenging. I think that’s why I never had a client refuse to let me teach the three-steps. And that’s why I’m sharing it with you now.
Step one is to feel the feeling. Feelings come around for a reason. We need to notice them, feel them, and contemplate their meaning. The big questions here are: How can you honor and feel your feelings? What can you do to respect your own feelings and listen to the underlying message? I’ve heard many answers. Here are a few. But you can generate your own list.
Frowning or crying if you feel sad
Grimacing and making angry faces into a mirror if you feel angry
Drawing an angry picture
Punching or kicking a pillow (no real violence though)
Going outside and yelling (or screaming into a pillow)
Scribbling on a note pad
Writing a nasty note to someone (but not delivering it)
Using your words, and talking to someone about what you’re feeling
Step two is to think a new thought or do something different. This step is all about intentionally doing or thinking something that might change or improve you mood. The big question here is: What can you think or do that will put you in a better mood?
I discovered that kids and adults have amazing mood-changing strategies. Here’s a sampling:
Tell a funny story (“Yesterday in math, my friend Todd farted”)
Tell a joke (What do you call it when 100 rabbits standing in a row all take one step backwards? A receding hare-line).
Tell a better joke (Why did the ant crawl up the elephant’s leg for the second time? It got pissed off the first time.)
Exercise!
Smile into a mirror
Talk to someone you trust
Put a cat (or a chicken or a duck) on your head
Chew a big wad of gum
I’m sure you get the idea. You know best what might put you in a good mood. When you’re ready, but not before, use your own self-knowledge to move into a better mood.
Step three is to spread the good mood. Moods are contagious. I’d say things like this to my clients:
“Emotions are contagious. Do you know what contagious means? It means you can catch emotions from being around other people who are in bad moods or good moods. Like when you got here. I noticed your mom was in a bad mood too. It made me wonder, did you catch the bad mood from her or did she catch it from you? Anyway, now you seem to be in a better mood. I’m wondering. Do you think you can make your mom “catch” your good mood?”
How do you share good moods? Saying “Cheer up” is off-limits. Here’s a short list of what I’ve heard from kids and adults.
Do someone a favor
Smile
Hold the door for a stranger
Offer a real or virtual hug
Listen to someone
Tell someone, “I love you”
Step four might be the best and most important step in the three-step emotional change trick. With kids, when I move on to step four, they always interrupt:
“Wait. You said there were only three steps!”
“Yes. That’s true. But because emotions are complicated and surprising, the three-step emotional change trick has four steps. The fourth step is for you to teach someone else the three steps.”
Why is it so easy to look for and focus in on that which annoys us . . . and so hard to look for and focus in on that which inspires us?
Nobody really knows the answer. There’s the usual speculation about evolution and potty training, but trying to find out “Why?” life is the way it is, is frustrating, as most 3-year-olds discover when they begin repeatedly asking their caregivers the Why question.
One thing is certain, if we want to focus on joy, inspiration, and small stuff that makes a positive difference, we have to be intentional. The default setting in most of our brains is to look for what’s wrong.
For this week’s Montana Happiness Challenge, we’re we’re encouraging everyone to intermittently and intentionally look for what’s right and good and inspiring. We know there is war, poverty, racism, climate change, and other big and horrible issues out there and we’re not suggesting you put your head in the sand and ignore these important problems. What we are suggesting is that you just direct your attention . . . a little more often . . . in the direction of the positive. #MHPHappinessChallenge #MontanaHappiness #WitnessInspiration
The research on mindsets is so immense that no one even bothers arguing about whether mindsets matter. They do. We all know it. Mindsets influence our performance, our success, and how we feel. That’s the good news.
The bad news is that it’s all-natural to automatically adopt negative mindsets. If you’re in a bad mood or mental state, you’ll find it easier to “see” things consistent with your bad mood.
The human psyche naturally and automatically looks for evidence to confirm what we already believe. At the same time, we tend to overlook, ignore, or dismiss whatever is inconsistent with our existing beliefs. Researchers and writers call this Confirmation bias.
Confirmation bias is everywhere, in everyone, and operating all the time. According to Brittanica.com, the formal definition is: “People’s tendency to process information by looking for, or interpreting, information that is consistent with their existing beliefs. This biased approach to decision making is largely unintentional, and it results in a person ignoring information that is inconsistent with their beliefs.” An example:
If you believe your parents or partner are hyper-critical of you, you will watch and listen for evidence to confirm your belief and be more likely to witness and experience them being critical. You will also tend to overlook or miss out noticing when they’re positive and affirming of you.
This week’s activity involves you intentionally shifting your mindset. Your goal is to look for small things that feel positive. In our University of Montana happiness class, we gave this assignment over Martin Luther King, Jr. weekend and called it: “Witness something inspiring.” We asked students to spend the weekend watching for inspirational moments in real life (not online). Students reported small and glorious outcomes, including:
A friend using good study skills
Watching my dog play in the yard
Seeing my co-worker treat a rude customer with respect
Noticing a high school student chat with a very old woman
Mindset shifting has other names. For example, in her book, Joyful, Ingrid Fetell Lee described “Joyspotting.” Joyspotting is a visual version of orienting yourself to that which brings you joy.
This week, your job is to intentionally watch, listen, and observe for things you find inspirational. If you don’t like the word inspirational, you can switch it out for joyspotting, and head out in search of joy. Although you could do an online search for “Inspirational,” we hope you’ll watch for inspiring or joyful moments in the real world.
What you notice may be small or big. The key point is to put your brain on intentional alert for that which will inspire or stimulate joy. Keep your sensory modalities open to the positive.
One warning: It’s natural to dismiss or disqualify small positive things you notice. You may see someone do something small (like hold open a door) and then quickly dismiss it as “no big deal.” For this week, try to avoid dismissing the small bright spots. Notice them, linger on them, and see what happens.
If you’re into the social media part of this challenge, we hope you’ll share your experiences. Using your favorite social media platform, consider sharing:
What it was like to intentionally watch for inspiration.
A description of what you observed.
Reactions you had to the inspirational event.
Anything else you want to add.
You can do this activity all on your own, or you can do it with a friend, a class, or a community.
Good luck . . . we look forward to your inspirational stories.
Back in the day, I was so into person-centered (aka nondirective) listening that I coauthored a 1989 article in the journal Teaching of Psychology titled, “Thou Shalt Not Ask Questions.” The point was that by temporarily eliminating questions from our therapeutic repertoire, we grow more aware of how to listen without using directive methods for facilitating client talk.
I’m still a fan of limiting therapist questions, if only to become more aware of their power. Even in the case of solution-focused or narrative therapies, when questions are the central therapeutic strategy, we should be as person-centered as possible when asking questions.
Below, I’ve included an excerpt of our coverage of listening from the forthcoming 7th edition of Clinical Interviewing. In the early 1990s, along with the first edition of Clinical Interviewing, we described a concept called the listening continuum. The excerpt starts there and then focuses in on what’s likely the most non-directive skill of all, therapeutic silence.
Here’s the excerpt. I hope you enjoy it and find it useful.
The Listening Continuum in Three Parts
Nondirective listening behaviors give clients responsibility for choosing what to talk about. Consistent with person-centered approaches, using nondirective behaviors is like handing your clients the reins to the horse and having them take the lead and choose where to take the session. In contrast, directive listening behaviors (Chapter 5) and directive action behaviors (Chapter 6) are progressively less person-centered. These three categories of listening behaviors (and the corresponding chapters) are globally referred to as the listening continuum. To get a visual sense of the listening continuum, see Table 4.1.
Nondirective Listening Behaviors on the LEFT Edge (Chapter 4)
Directive Listening Behaviors in the MIDDLE (Chapter 5)
Directive Action Behaviors on the RIGHT Edge (Chapter 6)
Attending behaviors or minimal encouragers
Feeling validation
Closed and therapeutic questions
Therapeutic silence
Interpretive reflection of feeling
Psychoeducation or explanation
Paraphrase
Interpretation (classic or reframing)
Suggestion
Clarification
Confrontation
Agreement/disagreement
Reflection of feeling
Immediacy
Giving advice
Summary
Open questions
Approval/disapproval
Urging
The ultimate goal is for you to use behavioral skills along the whole listening continuum. We want you to be able to apply these skills intentionally and with purpose. That way, when you review a video of your session with a supervisor, and your supervisor stops the recording and asks, “What exactly were you doing there?” you can respond with something like this:
I was doing an interpretive reflection of feeling. The reason I chose an interpretive reflection is that I thought the client was ready to explore what might be under their anger.
Trust us; this will be a happy moment for both you and your supervisor.
Hill (2020) organized the three listening continuum categories in terms of their primary purpose:
We hope you still (and will always) remember the Rogerian attitudes and have placed them firmly in the center of your developing therapeutic self. In addition, at this point we hope you understand the two-way nature of communication, the four different types of attending behaviors, and how your listening focus can shift based on a variety of factors, including culture and theoretical orientation.
Next, we begin coverage of technical skills needed to conduct a clinical interview. See Table 4.2 for a summary of nondirective listening behaviors and their usual effects. Having already reviewed attending behaviors, we now move to therapeutic silence.
Therapeutic Silence
Most people feel awkward about silence in social settings. Some researchers have described that therapists-in-training view silence as a “mean” response (Kivlighan & Tibbits, 2012). Despite the angst it can produce, silence can be therapeutic.
Therapeutic silence is defined as well-timed silence that facilitates client talk, respects the client’s emotional space, or provides clients with an opportunity to find their own voice regarding their insights, emotions, or direction. From a Japanese perspective,
Silence gives forgiveness and generosity to human dialogues in our everyday life. Without silence, our conversation tends to easily become too clever. Silence is the place where “shu”… (to sense the feeling of others, and forgive, show mercy, absolve, which represents an act of benevolence and altruism) arises, which Confucius said was the most important human attitude. (Shimoyama, 1989/2012, p. 6; translation by Nagaoka et al., 2013, p. 151)
Table 4.2 Summary of Nondirective Listening Behaviors and Their Usual Effects
Listening Response
Description
Primary Intent/Effect
Attending behaviors
Eye contact, leaning forward, head nods, facial expressions, etc.
Facilitates or inhibits client talk.
Therapeutic silence
Absence of verbal activity
Allows clients to talk. Provides “cooling off ” or introspection time. Allows clinician time to consider next response.
Paraphrase
Reflecting or rephrasing the content of what the client said
Assures clients that you heard them accurately and allows them to hear what they said.
Clarification
Restating a client’s message, preceded or followed by a closed question (e.g., “Do I have that right?”)
Clarifies unclear client statements and verifies the accuracy of what the clinician heard.
Reflection of feeling
Restatement or rephrasing of clearly stated emotion
Enhances clients’ experience of empathy and encourages further emotional expression.
Summary
Brief review of several topics covered during a session
Enhances recall of session content and ties together or integrates themes covered in a session.
Silence also allows clients to reflect on what they just said. Silence after a strong emotional outpouring can be therapeutic and restful. In a practical sense, silence also allows therapists time to intentionally select a response rather than rush into one.
In psychoanalytic psychotherapy, silence facilitates free association. Psychoanalytically oriented therapists use role induction to explain to clients that psychoanalytic therapy involves free expression, followed by occasional therapist comments or interpretations. Explaining therapy or interviewing procedures to clients is always important, but especially so when therapists are using potentially anxiety-provoking techniques, such as silence (Meier & Davis, 2020).
CASE EXAMPLE 4.2: EXPLAIN YOUR SILENCE
While on a psychoanalytically oriented internship, I (John) noticed one supervisor had a disturbing way of using silence during therapy sessions (and in supervision). He would routinely begin sessions without speaking. He sat down, looked at his client (or supervisee), and leaned forward expectantly. His nonverbal behavior was unsettling. He wanted clients and supervisees to free associate and say whatever came to mind, but he didn’t explain, in advance, what he was doing. Consequently, he came across as intimidating and judgmental. The moral of the story: Use role induction—if you don’t explain the purpose of your silence, you risk scaring away clients.
[End of Case Example 4.2]
Examples of How to Talk About Silence
Part of the therapist’s role involves skilled explanations of process and technique. This includes talking about silence. Case Example 4.2 is a good illustration of how therapist and client would have been better served if the therapist had explained why he started his sessions with silence.
Here’s another example of how a clinician might use silence therapeutically:
Katherine (they/them) is conducting a standard clinical intake interview. About 15 minutes into the session the client begins sobbing about a recent romantic relationship break-up. Katherine provides a reflection of feeling and reassurance that it’s okay to cry, saying, “I can see you have sad feelings about the break-up. It’s perfectly okay to honor those feelings in here and take time to cry.” They follow this statement with about 30 seconds of silence.
There are several other ways Katherine could handle this situation. They might prompt the client,
Let’s take a moment to sit with this and notice what emotions you’re feeling and where you’re feeling them in your body.
Or they might explain their purpose more clearly.
Sometimes it’s helpful to sit quietly and just notice what you’re feeling. And sometimes you might have emotional sensations in a particular part of your body. Would you be okay if we take a few moments to be quiet together so you can tune in to your emotions and where you’re feeling them?
In each of these scenarios, Katherine explains, at least briefly, the use of silence. This is crucial because when clinicians are silent, pressure is placed on clients to speak. When silence continues, the pressure mounts, and client anxiety may increase. In the end, clients may view their experience with an excessively silent therapist as aversive, lowering the likelihood of rapport and a second meeting.
Guidelines for Using Silence Therapeutically
Using silence may initially feel uncomfortable. With practice, you’ll increase your comfort level. Consider the following suggestions:
When a client pauses after making a statement or after hearing your paraphrase, let a few seconds pass rather than jumping in verbally. Given an opportunity, clients can move naturally into important material without guidance or urging.
As you’re waiting for your client to resume speaking, tell yourself that this is the client’s time for self-expression, not your time to prove you can be useful.
Try not to get into a rut regarding silence. When silence occurs, sometimes wait for the client to speak next and other times break the silence yourself.
Be cautious with silence if you believe your client is confused, psychotic, or experiencing an acute emotional crisis. Excessive silence and the anxiety it provokes can exacerbate these conditions.
If you feel uncomfortable during silent periods, use attending skills and look expectantly toward clients. This helps them understand it’s their turn to talk.
If clients appear uncomfortable with silence, give them instructions to free associate (e.g., “Just say whatever comes to mind”). Or you can use an empathic reflection (e.g., “It’s hard to decide what to say next”).
Remember, sometimes silence is the most therapeutic response available.
Read the interview by Carl Rogers (Meador & Rogers, 1984). It includes examples of how Rogers handled silence from a person-centered perspective.
Remember to monitor your body and face while being silent. There’s a vast difference between a cold silence and an accepting, warm silence. Much of this difference results from body language and an attitude that welcomes silence.
Use your words to explain the purpose of your silence (e.g., “I’ve been talking quite a lot, so I’m just going to be quiet here for a few minutes so you can have a chance to say whatever you like”). Clients may be either happy or terrified at the chance to speak freely.
John Wiley and Sons recently informed me of the excellent and exciting news that the 7th edition of Clinical Interviewing (CI7) has gone to press and will drop in the U.S. on or before September 30. Our wish for this edition is the same as previous editions: To provide research-based, theoretically supported, clinically insightful, and culturally informed education and training on how to conduct basic and advanced clinical interviews.
The Resource
Part of CI7 includes video updates. Most of the updates offer greater representation of culturally diverse counselors and psychotherapists. For example, the video link below features Dr. Devika “Dibya” Choudhuri describing a “grounding” technique that she uses when conducting tele-mental health (aka virtual) clinical interviews, the topic of Chapter 14.
Although you may have your own approaches to facilitating grounding during tele-mental health sessions, I believe Dr. Choudhuri’s idea is innovative and may be a resource that you can add to your toolkit.
Stay tuned, because over the next several weeks I’ll be posting additional fresh new text and video content from CI7.
The Request
Traditionally, publishers ask authors to gather promotional endorsements for new books. This time around, maybe because it’s the 7th edition, neither Wiley nor the absent-minded authors of CI7 thought about gathering endorsements. In the past, we’ve had Derald Wing Sue, John Norcross, Victor Yalom, Pamela Hays, Barbara Herlihy, Allen Ivey, David Jobes, and Marianne and Jerry Corey write short blurbs. Here’s what Derald Wing Sue said about the 6th edition:
The most recent edition of Clinical Interviewing is simply outstanding. It not only provides a complete skeletal outline of the interview process in sequential fashion, but fleshes out numerous suggestions, examples, and guidelines in conducting successful and therapeutic interviews. Well-grounded in the theory, research and practice of clinical relationships, John and Rita Sommers-Flanagan bring to life for readers the real clinical challenges confronting beginning mental health trainees and professionals. Not only do the authors provide a clear and conceptual description of the interview process from beginning to end, but they identify important areas of required mastery (suicide assessment, mental status exams, diagnosis and treatment electronic interviewing, and work with special populations). Especially impressive is the authors’ ability to integrate cultural competence and cultural humility in the interview process. Few texts on interview skills cover so thoroughly the need to attend to cultural dimensions of work with diverse clients. This is an awesome book written in an engaging and interesting manner. I plan to use this text in my own course on advanced professional issues. Kudos to the authors for producing such a valuable text.
―Derald Wing Sue, Ph.D., Professor of Psychology and Education, Teachers College, Columbia University
This time around, we’re less than two weeks from publishing and are without formal endorsements. As a consequence, I’m asking: “Is there ANYBODY out there who has read a portion of the CI7 manuscript or used a previous edition, who would like to share their thoughts about how the book influenced you or how the videos helped with your training?
[I know this last paragraph sounds pathetic. However, if you know me, you probably know my sense of humor, and the “Is there anybody out there?” call is BOTH a sincere request for your input AND me mocking myself for making this request.]
To be completely serious: If you want to share something positive about your experience—from any point in time—with the Clinical Interviewing text, I hope you’ll write a sentence or two or three (you don’t have to write half a page, like Derald Wing Sue) on the particular ways in which you found the book and/or videos meaningful to you.
To share your thoughts on any edition of the text, please post them here on this blog, or send them to me at john.sf@mso.umt.edu.
Thanks very much for considering this request. Please, please, I hope someone “out there” is listening!
I’ll be online in about 75 minutes to present a workshop for the TexChip folks from TAMU-CC. The title of the workshop is: “Tough Kids, Cool Counseling: Strategies for Engaging and Influencing Youth.”
Here’s the link to the workshop . . . where the CEUs are free!:
You may be aware of the irony in the workshop title. . . which is the fact that very soon into the workshop I tell everyone that we should never even “think” the words “Tough kids.” The reason we drop the terminology “Tough kids” is because it blames and labels the young people with whom we’re working, and they may sense that. Instead, all we have are “Kids in tough situations” and one of the tough situations is being in counseling or therapy.
Whether I’ll see you in 75 minutes or not, here are the ppts:
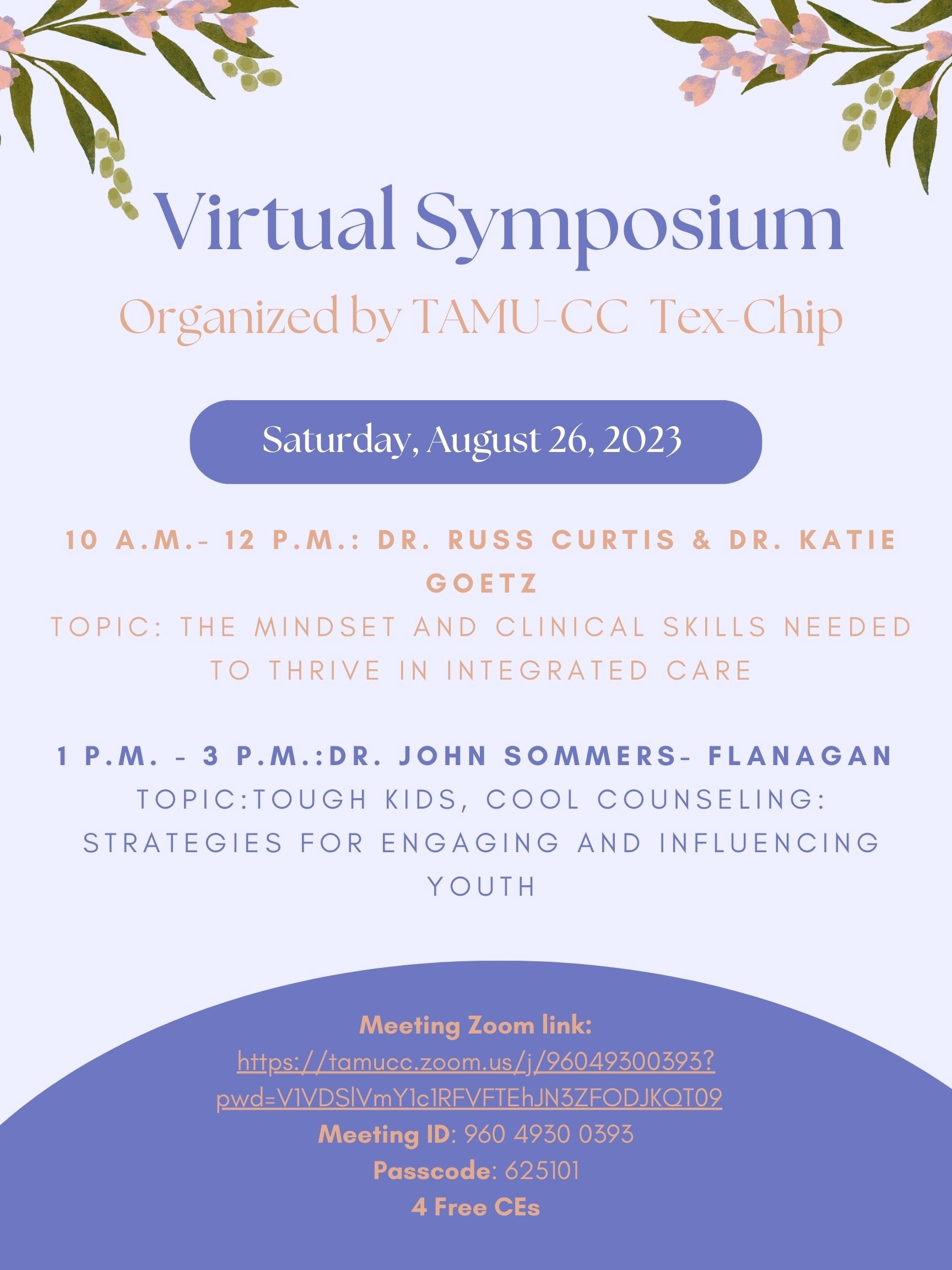
As a part of a virtual symposium offered by Texas A&M University – Corpus Christi, this coming Saturday, August 26, I’m doing a 2-hour free continuing education workshop from 12-2pm Mountain time (2pm-4pm Eastern). The cool thing is that the CEUs for this workshop are FREE. The less cool thing is that the workshop is on a Saturday.
My talk is: Tough Kids, Cool Counseling: Strategies for Engaging and Influencing Youth. Even better, I’ll be preceded by Dr. Russ Curtis and Dr. Katie Goetz (9am-11am Mountain time), who are presenting a 2-hour workshop on The Mindset and Clinical Skills Needed to Thrive in Integrated Care. . . and that’s 2 more FREE CEUs.
Below, I’ve pasted the blurbs and Zoom information for these online workshops.
You are invited to join Tex-Chip Virtual Symposium on Saturday, August 26, 2023, at 10am – 3pm (CST).
Dr. Russ Curtis & Dr. Katie Goetz is scheduled to present from 10am – 12pm CST on “The Mindset and Clinical Skills Needed to Thrive in Integrated Care.” In this interactive presentation, participants will learn how to integrate clinical skills with enlightening philosophical premises to expand their understanding of providing inclusive whole-person care. Attendees will develop their clinical voice through lecture, case examples, and discussions to begin asking the right questions about how to provide next-generation integrated care.
Dr. Sommers-Flanagan is scheduled to present from 1pm – 3pm CST on “Tough Kids, Cool Counseling: Strategies for Engaging and Influencing Youth.” Engaging “tough kids” in behavioral health can be immensely frustrating or splendidly gratifying. The truth of this statement is so obvious that the supportive reference, at least according to many teenagers is “Duh!” In this 2-hour workshop, participants will learn, experience, and practice several strategies for engaging and influencing youth. Several cognitive, emotional, and constructive brief counseling techniques will be described and demonstrated. Examples include acknowledging reality, positive questioning, wishes and goals, the affect bridge, the three-step emotional change trick, what’s good about you?/asset flooding, and more. Essential counseling principles, countertransference, and cultural issues will be included.
Hardly anyone with common sense or social skills ever argues about whether or not relationship factors are crucial to effective counseling and psychotherapy. Nevertheless, some scientists are reluctant to put relationship factors on par with counseling and psychotherapy techniques or procedures. IMHO, relationship factors are every bit as essential as so-called empirically-supported treatments.
This post is a pitch. Or it might be a pitch in a post. Either way, I am honored to share with you a hot-off-the-presses new book, titled Relationship Factors in Counseling, by Dr. Kimberly Parrow. Here’s the publisher’s link: https://titles.cognella.com/relationship-factors-in-counseling-9781793578754. The book is also available on Amazon and other booksellers.
Below, I’m pasting the Foreword to this book. Not only am I jazzed about the book, I’m also jazzed about the Foreword. You should read it. It’s really good. You’ll learn about Kimberly Parrow, as well as a bit of trivia about relationship factors that you should definitely know. I haven’t mentioned who wrote the Foreword, but I’m sure you’ll figure it out.
I first met Kimberly Parrow, before she was Dr. Kimberly Parrow, in a letter of recommendation from a psychology professor at the University of Montana. Having read well over 1,000 letters of recommendation over the years, this one imprinted in my brain. The professor wrote something like, “Kimberly Parrow is the real deal. You should admit her to master’s program in clinical mental health counseling. You will never regret it.”
We did (admit her into our master’s program . . . and our doctoral program). And we didn’t (ever regret it).
Kim Parrow was, is, and continues to be one of the most enthusiastic learners I’ve encountered. She walked onto our campus at 44-years-old, as a first-generation college student, having waited with bated breath for the money and opportunity to pursue her college degree. Nine years later she strolled off campus with her bachelor’s, master’s, and doctoral degrees. If we were Notre Dame, we’d call her a triple domer (n.b., that’s what you call people with three degrees from Notre Dame). At the University of Montana, we just call her amazing.
In one of her first doctoral classes, I introduced Kim to the concept of evidence-based relationship factors (EBRFs). She was hooked; hooked in the way that only graduate students get hooked. She was hooked by an idea. So hooked that she immediately wanted more; she wanted to write a journal article on EBRFs (so we did). She wanted to do her dissertation on EBRFs (so she did). She wanted to do extra additional trainings for practicum and internship students on EBRFs (and so she did). Kim’s attraction to EBRFs stemmed from her belief that relationships constitute the core of what’s therapeutic. As we explored EBRFs together, noting all the research supporting the idea that relationships drive counseling and psychotherapy, I came to see that Kim’s judgment was, and continues to be, practically perfect.
I’ve been reading dissertations for 30+ years. I’m embarrassed to say that I find reading most dissertations—even those written by students whom I love—drudgery. But Kim’s dissertation was electric. Page by page, she kept surprising me with new content and new learning; it was more than I expected. Kim had taken the basic knowledge and skills linked to EBRFs, contextualized them within the scientific literature, and then wrote about them in ways that inspired me to keep reading and keep learning. As she wrote more, her writing got better and better, and the content more illuminating.
About a month ago, I was unable to make it to my initial lecture for an advanced counseling theories course. I asked Kim to fill in. She quickly said yes. I offered to pay her. She quickly said no. To stick with the money theme, if I now had a dollar for every time one of my students has, since Kim’s lecture, mentioned Kim Parrow, eyes agog, and referenced the central role of relationship factors in counseling and psychotherapy, I would have many dollars. What I’m trying to say is that Kim is a natural and talented clinician-teacher. That’s a rare version of the real deal her former developmental psychology professor was trying to tell us about.
And now, a few words about this book. Kim has done what most scholars and professionals are unable to do. She has taken theoretical principles, empirical research findings, blended them with her common-sense-salt-of-the-earth style, and created a practical guide for helping counselors and psychotherapists be better. The book is aimed to slide into the educational development of practicum and/or internship students who have learned microskills and are facing their first clients. This particular point in student development is crucial; it’s a time when students sometimes lose their way as they try to make the improbable leap from microskills to counseling and psychotherapy techniques. In making that leap, they often fall prey to the urge to quickly “prove up” and “do something” with clients. In this process, they often abandon their microskills and forget about the therapeutic relationship. Kim’s overall point is this: Don’t forget about the therapeutic relationship because relationship factors are every bit as evidence-based as theory-based or research-based technical strategies. The renowned writer-researcher John C. Norcross put it this way:
Anyone who dispassionately looks at effect sizes can now say that the therapeutic relationship is as powerful, if not more powerful, than the particular treatment method a therapist is using.
The fact that therapeutic relationships are empirically supported makes Kim’s content relevant not only to students early in their clinical development, but also to all of us. Having taught this content with Kim, and to groups of professional counselors, psychologists, and social workers across the United States, I can say without hesitation that the content in this book can and will make all of us better therapists.
Kim covers 10 specific, evidence-based interactive relationship skills. What unique—and possibly the best thing about Kim’s coverage of relationship skills—is that she provides specific, actionable guidance for how to enact these 10 skills. As a preview, the 10 skills include:
Cultural humility
Congruence
Unconditional Positive Regard
Empathic Understanding
The Emotional Bond
Mutual Goal-Setting
Collaborative Therapeutic Tasks
Rupture and Repair
Countertransference Management
Progress Monitoring
In the pages that follow, you will get a taste of Kim Parrow’s relational orientation and a glimpse of the evidence supporting these 10 relationship factors as therapeutic forces that innervate counseling process. You will also experience the magic of a talented clinician-teacher. The magic—or, if you prefer, secret sauce—is Kim’s ability to make these distant intellectual relationship concepts real, practical, and actionable. To help make relationship concepts real, she has engaged several contributers (and herself) to write pedagogical break-out boxes titled, “Developing Your Skills.” Engaging with these skill development activities will, as the neuroscience fans like to say, “Change your brain” and help you develop neural pathways to enhance your relational connections.
As I write about skills and skill development, I’m aware that Carl (and Natalie) Rogers would view the reduction of his core conditions to “skills” as blasphemy. This awareness makes me want to emphasize that Kim “gets” Rogerian core conditions and does not reduce them into simple skills. Instead, she embraces the attitudinal and intentional dimensions of Rogerian core conditions, while simultaneously offering behaviors and words that counselors and psychotherapists can try on in hopes of expressing congruence, unconditional positive regard, and empathy.
I’ve had a few conversations with Derald Wing Sue over the years and he has always emphasized that culture in counseling and psychotherapy shouldn’t be relegated to a separate chapter at the end of the book—as if culture is ever a separate or standalone issue. Reading how Kim handles culture reminded me of Derald Wing Sue’s message. Instead of relegating it to the end, Kim begins with the relationship factor of cultural humility. That makes for a beautiful start. Cultural humility involves, above all else, the adoption of a non-superiority interpersonal stance. . . which is a simple and excellent anti-racist message. But Kim doesn’t stop talking about culture after Chapter 1. She does what Derald Wing Sue recommends: She integrates cultural awareness, knowledge, and skill development into the whole book. This stance—non-superiority and anti-racist—is consistent with Kim’s interpersonal style and is also the right place to start as counselors set about the journey to collaborate and co-create positive outcomes.
One of Kim’s writing goals is to offer ideas and activities that are likely to increase counselor cognitive complexity. You can see that in the two preceding paragraphs. Instead of reducing Rogerian core conditions into skills, she honors how they can become both attitudes and skills. And instead of putting culture into a silo, she spreads seeds of culture through all her chapters.
This book is a remarkable accomplishment. The language, the examples, the science, the skill development activities, and the tone, welcome readers to engage with this book, and bring the material to life. I believe if you read this book and engage in the activities, your counselor self-efficacy will grow.
For anyone who has gotten this far in reading this foreword, I have some reading tips to share. First, read this book with your heart wide open. I say this because this book is about the heart of the counselor or psychotherapist. Second, as you read, keep yourself in relationship with Kim. The book is about relational factors and the details Kim shares will not only help you in your relationships with clients, but, as she often reminded me and other people whom she cornered so she could talk to us about relational factors, these relationship factors are relevant and applicable to all relationships.
Obviously, I respect Dr. Kimberly Parrow and believe she has produced an excellent book. Obviously, I think you should read this book and do as so many of us have already done, learn about evidence-based relationship factors from someone who is a remarkably talented clinician-teacher. To paraphrase what that developmental psychology professor wrote about Kim many years ago, you should accept Kim Parrow into your personal program of learning immediately, and begin learning from her as soon as you can. You will not regret it.
All my best to you in your counseling and psychotherapy work.
John Sommers-Flanagan
Missoula, Montana
The place to click if you want to learn about psychotherapy, counseling, or whatever John SF is thinking about.