Group class is rolling downstream so fast that I feel I’m riding down Niagara Falls in a barrel. Well, that might be me being dramatic. My personal drama partly explains why I’m so late blogging about week 2 of group class.
Much of the focus of week 2 was on Yalom’s 11 therapeutic factors. I think they’re subtle, powerful, and sneaky insightful. When I teach the 11 factors, I try to give as many concrete examples as possible. Here’s one:
I got asked to run two in-school groups for 5th graders. I had twins in group (one in each group). These were difficult groups. I had let the principal assign the members. I know, bad idea, especially because I knew better; pre-group screening was both optimal and ethical. I share this story because it’s a good one, but also because I can acknowledge that I make mistakes and am still a work in progress.
The twins identified themselves as evil and good. They seemed to be living up to their self-proclaimed identities. The evil twin (let’s call her Zoey) got “removed” from the first three group meetings. My rule was to remove students and send them back to class if they violated the group rules. Zoey was intermittently making aggressive physical contact. She ripped up some “Disney cards” I had given all the students, and threw them at me. In each case, I just said, “Zoey, you’ve broken a rule and you need to go back to your class.” There were small protests, but she would eventually stand up, leave group and go back to class.
The other part of the rule was to let anyone who had been removed from group back in group if they presented me with an apology note. Zoey became an efficient apology note writer.
Dear Mr. Jhon,
I am sorry I pushed Amber. I won’t push Amber again. Can I come back to group?
Zoey
At the beginning of session 4, as Zoey walking into group, I impulsively said something like, “Zoey! You are in so much trouble. You are in so much trouble that you have to serve our group treats today.” Zoey stared at me, sat down, and began her new journey to becoming a very nice, polite, and wonderful group member.
I repeated my “You’re in so much trouble Zoey” opening the next week. And the next. Zoey never again pushed anyone, she didn’t argue, she became shockingly pleasant and cooperative.
At the end of group, Zoey wrote me a “Good bye” note. It read:
Dr. Mr. Jhon,
I had fun in group. Thank you for coming to our school. I will miss you.
Zoey
With this story (and many others), we get a chance to glimpse the complexities of human behavior. Zoey’s story also gives us a chance to apply counseling theory to group dynamics. The theory that comes to mind for Zoey is related to Dreikurs’ and Adler’s ideas about the 4 psychological goals of children’s misbehavior. You can read about why children (and adults) misbehave here: https://johnsommersflanagan.com/2017/06/10/why-children-misbehave-the-adlerian-perspective/. But in group, the focus is less on the 4 goals, and more on the two overarching factors that will, most of the time, mitigate and sometimes eliminate the misbehavior. What are these overarching factors?
A sense of belonging
Feeling useful
With Zoey, I think she suddenly felt useful. She also got proactive attention in a sort of sarcastic message of her being in trouble. I thought the “You’re in big trouble” part was pretty clever. But the more important part was to give her a job. . . to help her feel useful . . . and along with that came belonging.
In some ways, the Zoey intervention was an individual intervention that helped her function in a group. That was important because Zoey had never been successful in any group. She hadn’t been on a team, in a choir, and she rarely succeeded in making it through the school day without an interpersonal incident. “Graduating” from our group, was a big deal for Zoey.
Beyond the Adlerian principles, the evil twin scenario includes glimpses of Yalom’s therapeutic factors. Can you identify which ones? Here’s the list:
- Instillation of hope
- Universality
- Imparting information
- Altruism
- The corrective recapitulation of the family group
- Development of socializing techniques
- Imitative behavior
- Interpersonal learning
- Group cohesiveness
- Catharsis
- Existential factors
I’m heading into class momentarily, and so I’ll add the following observation quickly.
At this point, my group students still think I know what I’m doing. We’ve engaged in several whole group and subgroup (fishbowl) group activities where I’m the leader. One student referred to me as “smooth.” As much as I like that compliment, I also recognize that me being smooth is completely related to the students being engaged and cooperative. Maybe we’re still in the honeymoon phase of our group class. Maybe the storming is yet to come? Maybe everyone feels they belong, and that they’re useful. I do work at helping everyone feel belonging and usefulness.
As the instructor, I know that referencing that storming can happen and articulating, in advance, how I usually address storming, can make storming less likely. None of the students are especially keen to be the first stormers. Everyone (probably) knows that no matter the nature and content of the storming, I will try to meet it with acceptance and an opportunity for the stormer to “tell us more” while taking responsibility for their feelings. Nevertheless, sooner or later, I will want to prompt them to storm, rather than hold in feelings of discontent.
One last thought. I am not always smooth. I am not always competent. I am not always emotionally centered and ready to be a good group counselor. Given those realities, I’m also aware that it will be even more important (than being smooth) for me to acknowledge my mistakes and be vulnerable enough for students to accept me as a role model who isn’t just interested in being smooth, but is also interested in being vulnerable.
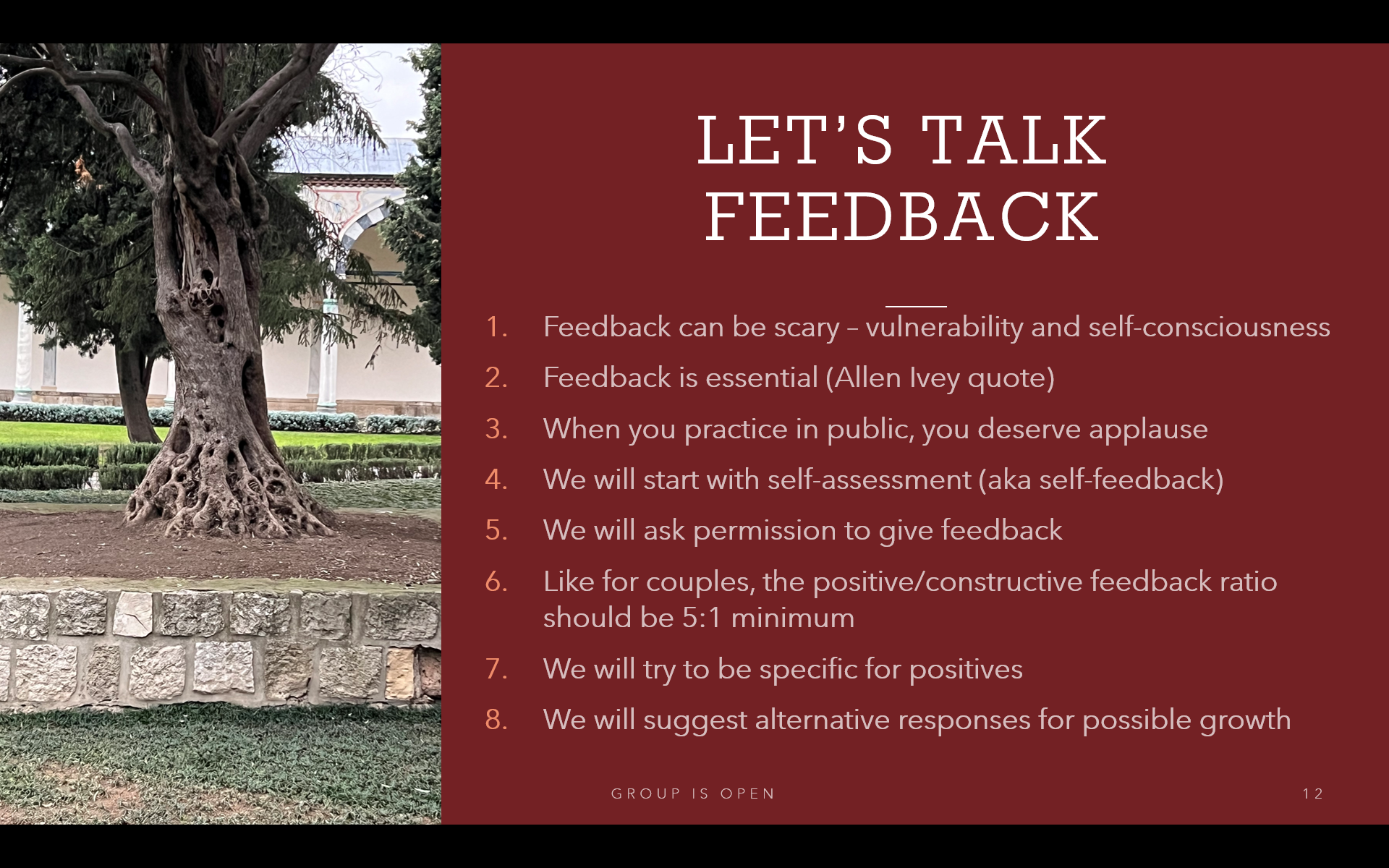
Thanks for reading! More to come soon. Here are the Week 2 powerpoints:
John